 Back
BackMuscular System - Anatomy & Physiology
You can tap to flip the card.
Control buttons has been changed to "navigation" mode.
1/24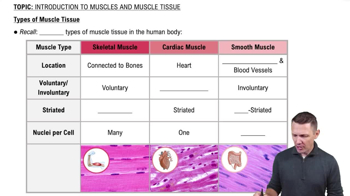
 6:31
6:31
Terms in this set (24)
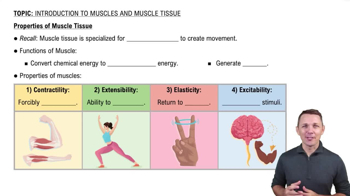
Contractility: ability to shorten
Extensibility: ability to stretch beyond resting length
Elasticity: ability to return to original length after stretching
Cardiac: involuntary, striated, heart walls
Smooth: involuntary, non-striated, walls of hollow organs
Perimysium: surrounds fascicles
Endomysium: surrounds individual muscle fibers
Insertion: attachment to bone that moves during contraction
2. Myosin binds actin forming crossbridge
3. Power stroke slides actin
4. ATP binds myosin to detach and repeat
Repolarization: K+ channels open, K+ exits restoring resting potential
Concentric: muscle shortens
Eccentric: muscle lengthens
Isometric: tension increases, length unchanged
Fast glycolytic: powerful, anaerobic
Fast oxidative: intermediate power and fatigue resistance
Resistance: increases fiber size, glycogen, converts fibers to fast glycolytic