 Back
BackArticulations (Joints): Structure, Function, and Clinical Relevance
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Chapter 8: Articulations (Joints)
Introduction to Joints (Articulations)
Joints, or articulations, are the locations where two or more bones meet. They play a critical role in movement, stability, and skeletal growth. The structure and function of joints are essential for understanding how the body moves and maintains its integrity.
Functions of Joints
Enable Movement: Muscles and tendons exert force across joints, allowing for a wide range of body movements.
Provide Stability: Some joints are designed for stability rather than movement, such as those in the skull, protecting underlying structures.
Allow Bone Growth: The epiphyseal plate (growth plate) is a temporary joint that enables long bones to lengthen during development.
Classification of Joints
Functional Classification
Synarthrosis: Immovable joints; provide maximum stability (e.g., sutures of the skull).
Amphiarthrosis: Slightly movable joints; offer both stability and limited movement (e.g., intervertebral discs).
Diarthrosis: Freely movable joints; allow a wide range of movements but are less stable (e.g., shoulder joint).
Structural Classification
Fibrous Joints: Bones joined by dense regular collagenous connective tissue; no joint cavity; mostly synarthroses or amphiarthroses.
Cartilaginous Joints: Bones joined by cartilage; no joint cavity; functionally synarthroses or amphiarthroses.
Synovial Joints: Bones separated by a fluid-filled joint cavity; always diarthroses (freely movable).
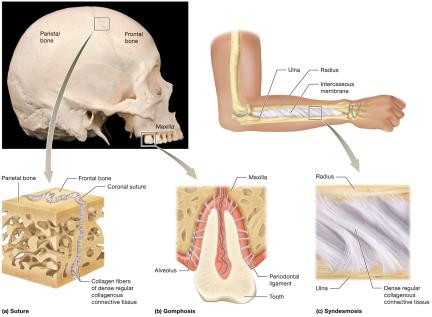
Fibrous Joints
Fibrous joints are united by collagen fibers, providing stability and permitting little or no movement.
Sutures: Found between skull bones; interlocking projections held by short collagen fibers. May fuse with age to form a synostosis.
Gomphoses: Joints between teeth and their sockets (alveoli) in the mandible or maxilla, stabilized by the periodontal ligament.
Syndesmoses: Bones joined by an interosseous membrane or ligament (e.g., between radius and ulna, tibia and fibula); allow limited movement.
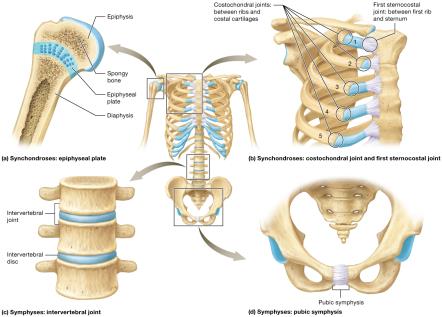
Cartilaginous Joints
Cartilaginous joints lack a joint cavity and allow little movement. They are classified based on the type of cartilage present.
Synchondroses: Bones united by hyaline cartilage; immovable (e.g., epiphyseal plate, first sternocostal joint, costochondral joints).
Symphyses: Bones united by a fibrocartilage pad; slightly movable (e.g., intervertebral discs, pubic symphysis).
Clinical Note: Epiphyseal Plate Fractures
The epiphyseal plate is a weak point in a child’s skeleton; fractures can lead to limb length discrepancies, deformities, or early arthritis if not properly managed.
Common causes include sports, accidents, and falls. Treatment ranges from immobilization to surgery.
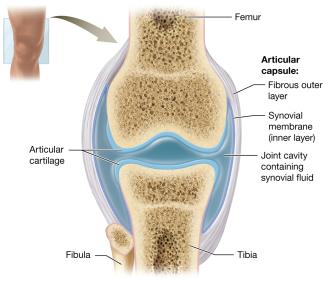
Synovial Joints
Synovial joints are the most common and movable type of joint in the body. They are characterized by a joint cavity filled with synovial fluid.
Articular Capsule: Double-layered; outer fibrous layer (dense irregular connective tissue) and inner synovial membrane (secretes synovial fluid).
Synovial Fluid: Lubricates, nourishes, and absorbs shock within the joint.
Articular Cartilage: Hyaline cartilage covering bone surfaces; reduces friction and absorbs shock.
Other Components: Adipose tissue (padding), blood vessels (nourishment), and nerves (pain and proprioception).
Stabilizing and Supportive Structures
Ligaments: Connect bone to bone; can be intrinsic (within capsule) or extrinsic (outside capsule).
Tendons: Connect muscle to bone; stabilize joints by maintaining muscle tone.
Bursae: Fluid-filled sacs that reduce friction in areas of high stress.
Tendon Sheaths: Elongated bursae that protect tendons in high-friction areas.
Clinical Note: Bursitis and Arthritis
Bursitis: Inflammation of a bursa, often due to trauma, repetitive motion, or disease. Symptoms include pain, swelling, and warmth.
Arthritis: Inflammation of joints, leading to pain and reduced mobility. Types include osteoarthritis (wear and tear), rheumatoid arthritis (autoimmune), and gouty arthritis (uric acid crystals).
Functional Classes of Synovial Joints
Synovial joints are classified by the number of axes around which bones can move:
Nonaxial: Movement in one or more planes, but not around an axis (e.g., intercarpal joints).
Uniaxial: Movement around one axis (e.g., elbow joint).
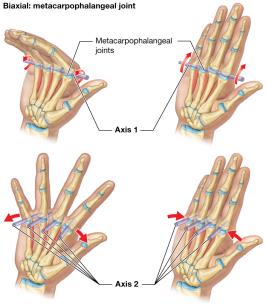
Biaxial: Movement around two axes (e.g., metacarpophalangeal joints).
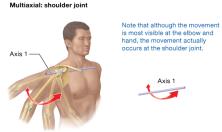
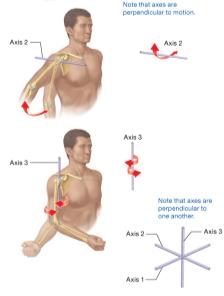
Multiaxial (Triaxial): Movement around three axes (e.g., shoulder joint).

Movements at Synovial Joints
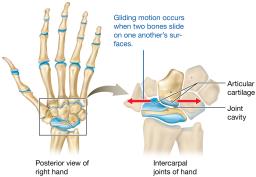
Gliding Movements
Sliding motion between flat surfaces of bones; nonaxial (e.g., intercarpal joints).
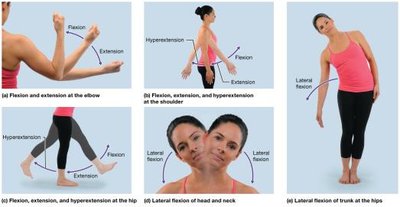
Angular Movements
Flexion: Decreases the angle between bones (e.g., bending the elbow).
Extension: Increases the angle between bones.
Hyperextension: Extension beyond anatomical position.
Lateral Flexion: Sideways movement (e.g., bending the trunk).
Abduction: Movement away from the midline.
Adduction: Movement toward the midline.
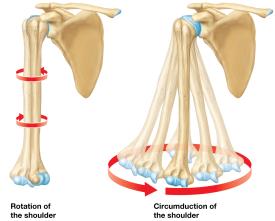
Circumduction: Circular movement combining flexion, extension, abduction, and adduction.

Rotation: Bone pivots around its own longitudinal axis.
Internal (Medial) Rotation: Toward the midline.
External (Lateral) Rotation: Away from the midline.

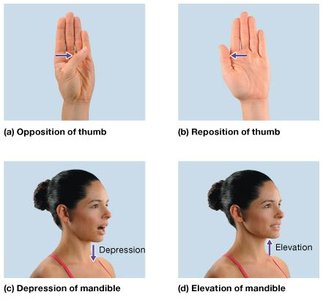
Special Movements
Opposition/Reposition: Movement of the thumb across the palm and back.
Depression/Elevation: Inferior and superior movement (e.g., opening and closing the mouth).
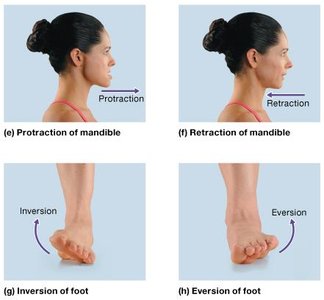
Protraction/Retraction: Anterior and posterior movement (e.g., jutting jaw forward and back).
Inversion/Eversion: Rotational movement of the foot inward or outward.
Dorsiflexion/Plantarflexion: Movement of the foot upward (toes toward head) or downward (toes toward ground).
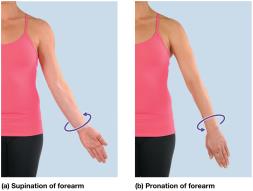
Supination/Pronation: Rotation of the forearm so the palm faces anteriorly (supination) or posteriorly (pronation).

Range of Motion
Determined by joint structure; nonaxial joints have the smallest range, multiaxial joints the greatest.
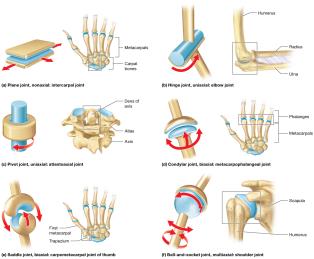
Structural Classes of Synovial Joints
Plane Joint: Nonaxial; flat surfaces (e.g., intercarpal joints).
Hinge Joint: Uniaxial; convex fits into concave (e.g., elbow).
Pivot Joint: Uniaxial; rounded surface fits into a groove (e.g., proximal radioulnar joint).
Condylar (Ellipsoid) Joint: Biaxial; oval convex fits into shallow concave (e.g., metacarpophalangeal joints).
Saddle Joint: Biaxial; each surface has both convex and concave regions (e.g., thumb carpometacarpal joint).
Ball-and-Socket Joint: Multiaxial; spherical head fits into a cup-like socket (e.g., shoulder, hip).
Specific Joints: Structure and Clinical Relevance
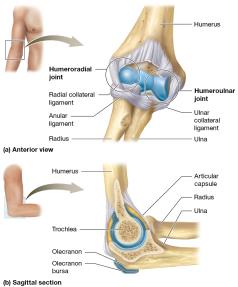
The Elbow Joint
Composed of the humeroulnar and humeroradial joints.
Stabilized by the radial (lateral) collateral, ulnar (medial) collateral, and anular ligaments.
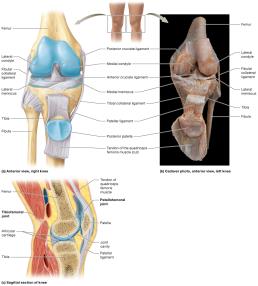
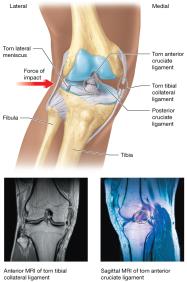
The Knee Joint
Largest diarthrosis; hinge joint with some rotation and gliding.
Composed of tibiofemoral and patellofemoral joints.
Stabilized by menisci, collateral ligaments, and cruciate ligaments (ACL and PCL).
Clinical Note: The Unhappy Triad
Lateral blows to the knee can rupture the tibial collateral ligament, lateral meniscus, and anterior cruciate ligament (ACL).
Common in contact sports; requires surgical repair and rehabilitation.
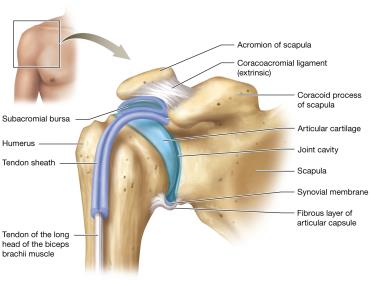
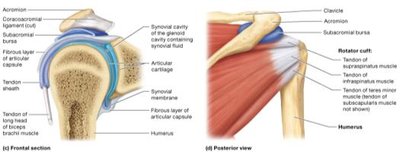
The Shoulder (Glenohumeral) Joint
Ball-and-socket joint; most freely movable but least stable.
Stabilized by the articular capsule, coracohumeral and glenohumeral ligaments, rotator cuff muscles, and bursae.
Glenoid labrum deepens the socket.

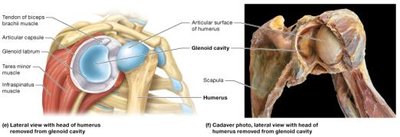
Clinical Note: Shoulder Dislocations
Dislocation involves the humeral head leaving the glenoid cavity; most common anteriorly and inferiorly.
Separated shoulder involves the acromioclavicular joint, not the glenohumeral joint.
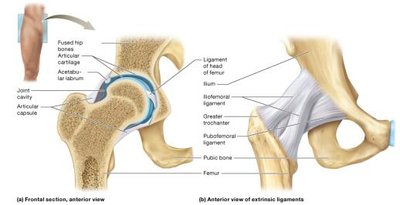
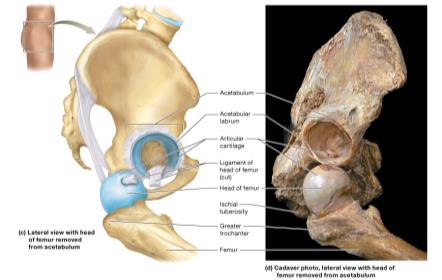
The Hip (Coxal) Joint
Ball-and-socket joint between the acetabulum and femoral head; more stable than the shoulder.
Stabilized by the acetabular labrum, strong articular capsule, and several ligaments (iliofemoral, ischiofemoral, pubofemoral, ligament of the head of femur).
Surrounded by large muscle groups for additional support.
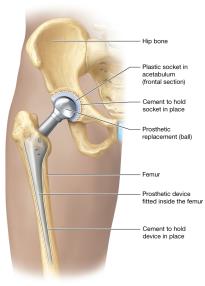
Clinical Note: Hip Joint Replacement
Indicated for severe arthritis, trauma, or bone tumors.
Total replacement involves both the femoral head and acetabulum; partial replacement involves only the femoral head.
Physical therapy is essential for recovery.
Summary Table: Joint Classification
Structural Class | Functional Class | Main Tissue | Example |
|---|---|---|---|
Fibrous | Synarthrosis/Amphiarthrosis | Dense regular connective tissue | Suture, syndesmosis, gomphosis |
Cartilaginous | Synarthrosis/Amphiarthrosis | Hyaline or fibrocartilage | Epiphyseal plate, pubic symphysis |
Synovial | Diarthrosis | Joint cavity with synovial fluid | Shoulder, knee, hip |
Key Terms and Concepts
Articulation: Joint between bones.
Synovial Fluid: Lubricating fluid in synovial joints.
Ligament: Connects bone to bone.
Tendon: Connects muscle to bone.
Bursa: Fluid-filled sac reducing friction.
Meniscus: Fibrocartilage pad in the knee.
Labrum: Fibrocartilage ring in shoulder and hip joints.
Additional info: This guide expands on the original lecture slides by providing definitions, clinical notes, and a summary table for clarity and exam preparation.
