 Back
BackAutonomic Agents: Mechanisms, Indications, and Clinical Applications
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
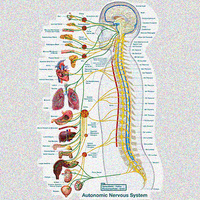
Autonomic Nervous System (ANS): Overview
Structure and Function
The autonomic nervous system (ANS) regulates involuntary physiological processes, including heart rate, blood pressure, respiration, digestion, and pupil diameter. It is divided into the sympathetic and parasympathetic nervous systems, each with distinct neurotransmitters and receptor types.
Sympathetic Nervous System (SANS): Prepares the body for 'fight or flight' responses.
Parasympathetic Nervous System (PANS): Promotes 'rest and digest' activities.
Ophthalmological Indications for ANS Drugs
Pupil Dilation and Constriction
Autonomic drugs are used to manipulate pupil size for diagnostic and therapeutic purposes. The iris contains two muscles: the radial muscle (dilates pupil) and the circular muscle (constricts pupil).
Phenylephrine (α1 agonist): Contracts the radial muscle, causing pupil dilation (mydriasis).
Cyclopentolate (muscarinic antagonist): Relaxes the circular muscle, also causing mydriasis.
Muscarinic agonists: Contract the circular muscle, causing pupil constriction (miosis).
Both drug types are typically administered topically.
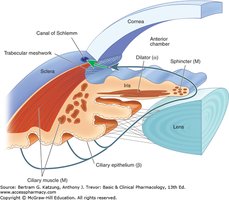
Glaucoma (Open Angle)
Glaucoma is associated with increased intraocular pressure due to impaired outflow of aqueous humor. ANS drugs can lower intraocular pressure by two main mechanisms:
Ciliary muscle contraction (muscarinic agonists): Increases tension on the trabecular meshwork, opening pores and enhancing aqueous humor outflow.
Beta blockers: Reduce aqueous humor secretion by blocking β-adrenoreceptors on the ciliary epithelium.
Cardiovascular Indications for ANS Drugs
Major Cardiovascular Diseases
ANS drugs are used in the management of several cardiovascular diseases, including:
Heart Failure
Angina Pectoris
Arrhythmia
Hypertension
Heart Failure
Heart failure is characterized by insufficient cardiac output to meet the body's needs. It can be classified as:
Systolic failure: Reduced contractility and ejection fraction.
Diastolic failure: Stiffness and impaired relaxation, leading to reduced filling and stroke volume.
Treatment goals differ for chronic and acute heart failure:
Chronic management: Reduce sympathetic overactivity, decrease afterload and preload, and minimize edema.
Acute episodes: Stimulate cardiac output with cardiotonic drugs (e.g., dobutamine, a β1 agonist).
Beta blockers are used in chronic heart failure to attenuate toxic effects of high sympathetic activity, reduce renin secretion, and improve ventricular filling time.
Angina Pectoris
Angina pectoris is chest pain caused by myocardial ischemia due to an imbalance between oxygen supply and demand. The main treatment goal is to decrease myocardial oxygen requirement by lowering heart rate, preload, afterload, and contractility.
Beta blockers: Reduce all determinants of myocardial oxygen demand.
Alpha-1 blockers: Lower preload and afterload but may trigger reflex increases in contractility, making them less ideal for angina.

Hypertension
Hypertension is defined as persistently elevated blood pressure. Blood pressure is determined by cardiac output (CO) and total peripheral resistance (TPR):
Where:
(Heart Rate × Stroke Volume)
ANS drugs lower blood pressure by:
Beta-1 blockers: Decrease contractility and renin secretion (reducing both CO and TPR via the RAAS pathway).
Alpha-1 blockers: Decrease TPR by relaxing vascular smooth muscle.
Arrhythmias and ANS Drug Intervention
Supraventricular Tachycardias (SVTs)
SVTs are arrhythmias originating above the ventricles, often involving the atria or AV node. The AV node acts as a gatekeeper, limiting the number of signals transmitted to the ventricles.

Beta blockers are used to slow AV node conduction and reduce heart rate, thereby controlling SVTs.
Cellular Basis of Arrhythmias
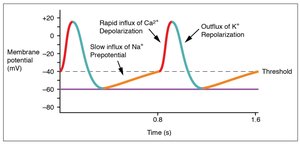
Arrhythmias can result from abnormal conduction velocity, refractory period, or automaticity. These properties are determined by the function of ion channels in cardiac cells.
Conduction velocity: Determined by the slope of Phase 0 (rapid depolarization) in the action potential.
Refractory period: Determined by the duration of Phase 3 (repolarization).
Beta Blockers in Arrhythmia
Beta blockers decrease conduction velocity and heart rate by reducing calcium influx and cAMP production in nodal cells. Sotalol, a beta blocker, also blocks potassium channels, increasing the refractory period and further suppressing arrhythmias.
Cholinergic Agents
Muscarinic Agonists
Muscarinic agonists selectively stimulate muscarinic cholinergic receptors, mimicking the effects of acetylcholine. They are classified as:
Synthetic choline esters: e.g., bethanechol, carbachol
Naturally occurring: e.g., pilocarpine

Muscarinic agonists increase glandular secretion, GI motility, and cause miosis and bradycardia. They are used to treat conditions such as glaucoma, xerostomia, and urinary retention.
Cholinesterase Inhibitors (ChE-Is)
ChE-Is inhibit the breakdown of acetylcholine, enhancing cholinergic transmission. They can be reversible (short- or long-acting) or irreversible (organophosphates).
Short-acting: Edrophonium (non-covalent binding)
Long-acting: Neostigmine, physostigmine (covalent but reversible binding)
Irreversible: Echothiophate, organophosphates (very stable covalent bonds)

Indications include myasthenia gravis, reversal of neuromuscular block, glaucoma, and Alzheimer's disease.
Adrenergic Agents
Adrenergic Agonists
Adrenergic agonists activate alpha and/or beta receptors. They are classified as:
Direct-acting: Epinephrine, norepinephrine, isoproterenol, phenylephrine, dobutamine, albuterol
Indirect-acting: Amphetamine, tyramine (increase endogenous neurotransmitter release)
Mixed-acting: Ephedrine, pseudoephedrine (direct receptor stimulation and neurotransmitter release)
Adrenergic Antagonists
Adrenergic antagonists block alpha and/or beta receptors, reducing sympathetic effects. They are used to treat hypertension, heart failure, arrhythmias, and benign prostatic hyperplasia (BPH).
Alpha blockers: Prazosin, terazosin, tamsulosin (selective for α1)
Beta blockers: Propranolol, metoprolol, atenolol, carvedilol, labetalol
Some beta blockers have additional properties, such as partial agonism (ISA), nitric oxide production, or combined alpha and beta blockade.
Summary Table: Major ANS Drug Classes and Actions
Drug Class | Main Receptor(s) | Key Effects | Clinical Indications |
|---|---|---|---|
Muscarinic Agonists | M1, M2, M3 | Increase secretion, GI motility, miosis, bradycardia | Glaucoma, xerostomia, urinary retention |
Cholinesterase Inhibitors | M, N | Enhance cholinergic transmission | Myasthenia gravis, Alzheimer's, glaucoma |
Adrenergic Agonists | α1, α2, β1, β2 | Vasoconstriction, bronchodilation, increased HR/contractility | Shock, asthma, nasal congestion |
Adrenergic Antagonists | α1, β1, β2 | Vasodilation, decreased HR/contractility | Hypertension, heart failure, BPH |
Additional info: This guide integrates pharmacological mechanisms with clinical applications, focusing on the physiological rationale for drug selection and side effects. Students should be able to predict drug effects based on receptor location and function.
