 Back
BackChapter 21: The Respiratory System – Structure, Function, and Physiology
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
The Respiratory System: Overview
Introduction
The respiratory system is essential for gas exchange, supplying oxygen to the body and removing carbon dioxide. It also plays roles in speech, olfaction, and homeostatic regulation of blood pH and pressure.
Major Functions: Gas exchange, sound production, olfaction, acid-base balance, and assistance in venous and lymphatic return.
Other Functions: Assists in defecation, urination, childbirth, and synthesizes enzymes for blood pressure regulation.
Anatomy of the Respiratory System
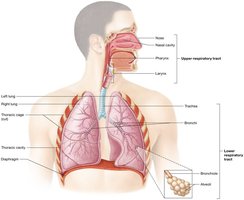
Upper and Lower Respiratory Tracts
The respiratory system is divided into upper and lower tracts, each with specialized structures for air conduction and gas exchange.
Upper Respiratory Tract: Nose, nasal cavity, pharynx, and larynx.
Lower Respiratory Tract: Trachea, bronchi, bronchioles, and lungs.
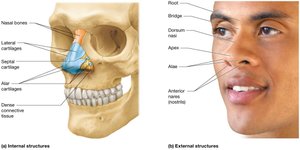
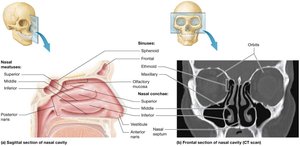
The Nose and Nasal Cavity
The nose is the primary entryway for air, supported by bone and cartilage, and lined with mucosa to filter, warm, and humidify incoming air.
External Anatomy: Includes root, bridge, dorsum nasi, apex, alae, and nostrils (anterior nares).
Internal Anatomy: Nasal septum, conchae, and meatuses increase surface area for air processing.
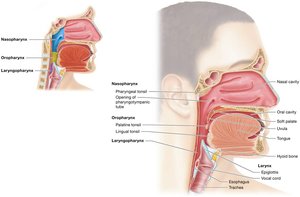
The Pharynx
The pharynx is a muscular tube that serves as a passageway for both air and food, divided into three regions: nasopharynx, oropharynx, and laryngopharynx.
Nasopharynx: Air passageway, contains pharyngeal tonsil.
Oropharynx: Passage for food and air, contains palatine and lingual tonsils.
Laryngopharynx: Connects to larynx and esophagus.
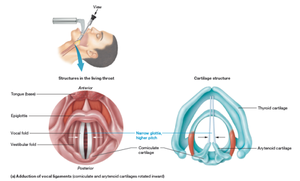
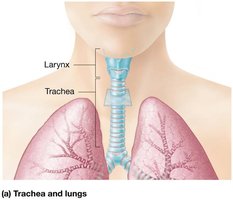
The Larynx
The larynx, or voice box, is responsible for sound production and protecting the lower airways during swallowing. It is composed of nine cartilages, including the thyroid, cricoid, arytenoid, corniculate, and cuneiform cartilages.
Thyroid Cartilage: Largest, forms the Adam's apple.
Epiglottis: Prevents food from entering the airway.
Vocal Ligaments: Vibrate to produce sound; pitch and loudness depend on tension and force of air.

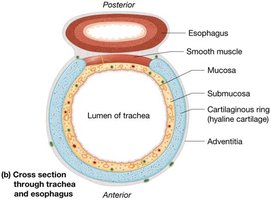
The Trachea
The trachea, or windpipe, is a tube supported by C-shaped hyaline cartilage rings, lined with pseudostratified ciliated columnar epithelium and goblet cells for mucus production and debris removal.
Carina: Last tracheal cartilage; triggers cough reflex.
Function: Conducts air to bronchi; mucociliary escalator removes particles.
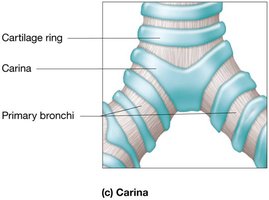
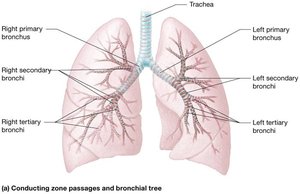
The Bronchial Tree
The bronchial tree consists of branching airways that conduct air from the trachea to the alveoli. It includes primary, secondary, and tertiary bronchi, bronchioles, and terminal bronchioles.
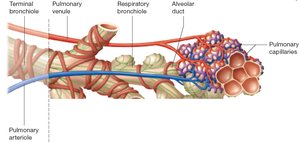
Respiratory Bronchioles: Lead to alveolar ducts and alveolar sacs, where gas exchange occurs.
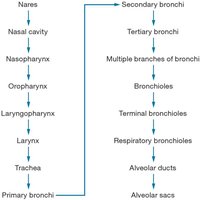
Pathway of Air
Air passes through a series of structures before reaching the alveoli for gas exchange.
Conducting Zone: Nares → Nasal cavity → Pharynx → Larynx → Trachea → Bronchi → Bronchioles
Respiratory Zone: Respiratory bronchioles → Alveolar ducts → Alveolar sacs
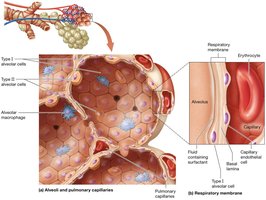
Alveoli and the Respiratory Membrane
Alveoli are tiny air sacs where gas exchange occurs. The respiratory membrane consists of alveolar epithelium, fused basement membrane, and capillary endothelium, allowing efficient diffusion of gases.
Type I Alveolar Cells: Simple squamous cells for gas exchange.
Type II Alveolar Cells: Secrete surfactant to reduce surface tension.
Alveolar Macrophages: Remove debris and pathogens.
The Lungs and Pleurae
The lungs are paired organs divided into lobes and surrounded by pleural membranes. The pleurae produce fluid to reduce friction during breathing.
Visceral Pleura: Covers the lungs.
Parietal Pleura: Lines the thoracic cavity.
Pleural Cavity: Contains pleural fluid.
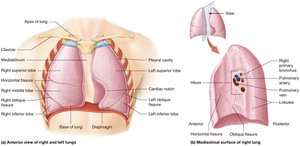
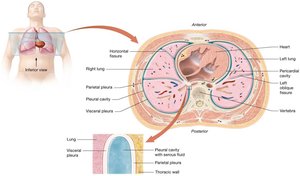
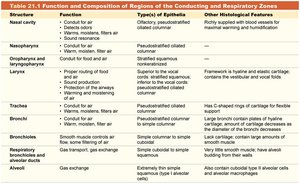
Table: Function and Composition of Regions of the Conducting and Respiratory Zones
Structure | Function | Type(s) of Epithelia | Other Histological Features |
|---|---|---|---|
Nasal cavity | Conducts, filters, warms, moistens air | Olfactory, pseudostratified ciliated columnar | Richly supplied with blood vessels and mucous glands |
Nasopharynx | Conduit for air | Pseudostratified ciliated columnar | --- |
Oropharynx and laryngopharynx | Conduit for food and air | Stratified squamous | --- |
Larynx | Voice production, air passage | Pseudostratified ciliated columnar | Framework is hyaline and elastic cartilage |
Trachea | Conduit for air, filters air | Pseudostratified ciliated columnar | Hyaline cartilage rings for flexibility |
Bronchi | Conduit for air, filters air | Simple columnar to simple cuboidal | Large bronchi contain plates of hyaline cartilage |
Bronchioles | Conduit for air, gas exchange | Simple cuboidal | Large amounts of smooth muscle |
Respiratory bronchioles | Gas transport, gas exchange | Simple cuboidal | --- |
Alveoli | Gas exchange | Extremely thin simple squamous | Alveolar macrophages, surfactant-secreting cells |
Pulmonary Ventilation
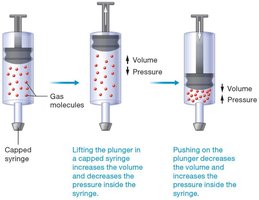
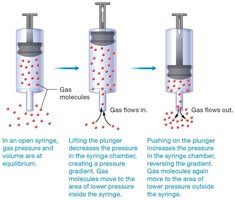
Pressure–Volume Relationship (Boyle’s Law)
Pulmonary ventilation (breathing) involves inspiration and expiration, driven by pressure gradients created by changes in lung volume. Boyle’s law states that at constant temperature, the pressure and volume of a gas are inversely related:
Inspiration: Volume increases, pressure decreases, air flows in.
Expiration: Volume decreases, pressure increases, air flows out.
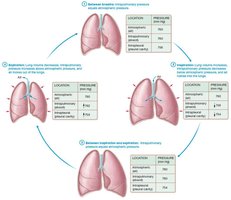
Pressure Gradients in Pulmonary Ventilation
Three main pressures influence ventilation:
Atmospheric Pressure: Pressure of air outside the body (about 760 mm Hg at sea level).
Intrapulmonary Pressure: Pressure within alveoli; equalizes with atmospheric pressure.
Intrapleural Pressure: Pressure within pleural cavity; always slightly less than intrapulmonary pressure, creating a vacuum that keeps lungs inflated.
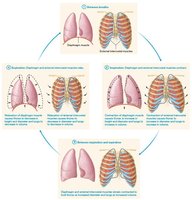
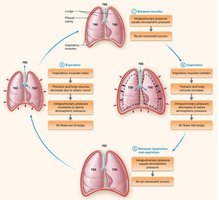
Mechanics of Inspiration and Expiration
Inspiration is an active process involving contraction of the diaphragm and external intercostal muscles. Expiration is usually passive, relying on elastic recoil of lung tissue and relaxation of inspiratory muscles.
Diaphragm: Main muscle of inspiration.
External Intercostals: Elevate ribs to expand thoracic cavity.
Expiration: Diaphragm relaxes, lung volume decreases, air is expelled.
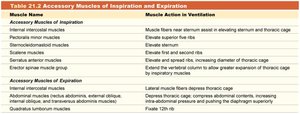
Accessory Muscles of Inspiration and Expiration
Muscle Name | Muscle Action in Ventilation |
|---|---|
Internal intercostal muscles | Depress thoracic cage (expiration) |
Sternocleidomastoid | Elevates sternum (inspiration) |
Scalene muscles | Elevate first and second ribs (inspiration) |
Rectus abdominis, external and internal obliques, transversus abdominis | Compress abdominal contents, push diaphragm superiorly (expiration) |
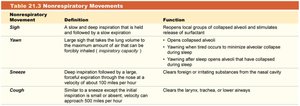
Nonrespiratory Movements
Nonrespiratory Movement | Definition | Function |
|---|---|---|
Sigh | Slow, deep inspiration held and followed by slow expiration | Reopens local groups of collapsed alveoli |
Yawning | Large sigh that takes lung volume to maximum | Opens collapsed alveoli |
Sneeze | Deep inspiration followed by forceful expiration through nose | Clears foreign substances from nasal cavity |
Cough | Deep inspiration followed by forceful expiration through mouth | Clears larynx, trachea, or lower airways |
Physical Factors Influencing Pulmonary Ventilation
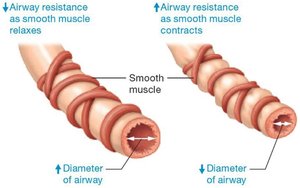
Airway Resistance
Airway resistance is determined by the diameter of bronchioles, which is regulated by smooth muscle contraction and relaxation.
Bronchodilation: Increases airway diameter, decreases resistance, increases airflow.
Bronchoconstriction: Decreases airway diameter, increases resistance, decreases airflow.
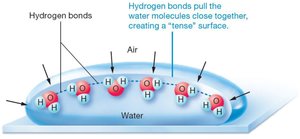
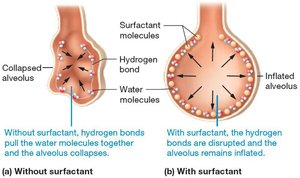
Alveolar Surface Tension and Surfactant
Surface tension at the air-water interface in alveoli tends to collapse alveoli. Surfactant, produced by type II alveolar cells, reduces surface tension and prevents alveolar collapse.
Without Surfactant: Alveoli collapse due to hydrogen bonding of water molecules.
With Surfactant: Disrupts hydrogen bonds, keeping alveoli open.
Pulmonary Compliance
Pulmonary compliance is the ability of the lungs and chest wall to stretch. It is influenced by alveolar surface tension, elasticity of lung tissue, and mobility of the chest wall.
High Compliance: Lungs expand easily.
Low Compliance: Lungs are stiff and resist expansion.
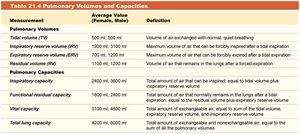
Pulmonary Volumes and Capacities
Measurement of Pulmonary Function
Pulmonary volumes and capacities are measured using a spirometer. Key volumes include:
Tidal Volume (TV): Air exchanged during normal breathing.
Inspiratory Reserve Volume (IRV): Maximum air inhaled after normal inspiration.
Expiratory Reserve Volume (ERV): Maximum air exhaled after normal expiration.
Measurement | Average Value (Female, Male) | Definition |
|---|---|---|
Tidal volume (TV) | 500 mL, 500 mL | Volume of air exchanged with normal, quiet breathing |
Inspiratory reserve volume (IRV) | 1900 mL, 3100 mL | Maximum volume of air that can be forcibly inspired after a tidal inspiration |
Expiratory reserve volume (ERV) | 700 mL, 1200 mL | Maximum volume of air that can be forcibly expired after a tidal expiration |
Vital capacity | 3100 mL, 4800 mL | Total amount of air that can be exchanged voluntarily |
Total lung capacity | 4200 mL, 6000 mL | Total amount of air the lungs can hold |
Gas Exchange
Dalton’s Law of Partial Pressures
Each gas in a mixture exerts its own pressure, and the total pressure is the sum of all partial pressures. Gases diffuse from areas of higher to lower partial pressure.
Henry’s Law
The amount of gas dissolved in a liquid is proportional to its partial pressure and solubility. Oxygen is more soluble in plasma than nitrogen, while carbon dioxide is the most soluble.
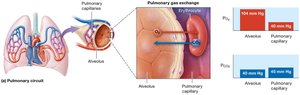
Pulmonary Gas Exchange (External Respiration)
Oxygen diffuses from alveoli into pulmonary capillaries, while carbon dioxide diffuses in the opposite direction. The efficiency depends on partial pressure gradients, surface area, membrane thickness, and ventilation-perfusion matching.
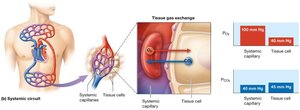
Tissue Gas Exchange (Internal Respiration)
Oxygen diffuses from systemic capillaries into tissues, and carbon dioxide diffuses from tissues into blood. Driven by differences in partial pressures.
Gas Transport in Blood
Oxygen Transport
Most oxygen is transported bound to hemoglobin (Hb) in erythrocytes. Each Hb molecule can carry four oxygen molecules. Loading occurs in the lungs; unloading occurs in tissues.
Oxygen-Hemoglobin Dissociation Curve: Shows the relationship between PO2 and hemoglobin saturation.
Bohr Effect: Increased acidity and PCO2 decrease Hb affinity for oxygen, enhancing unloading in tissues.

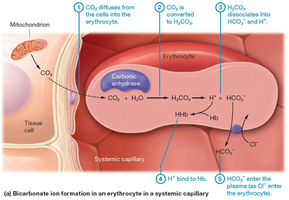
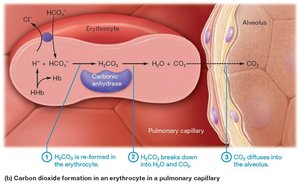
Carbon Dioxide Transport
CO2 is transported in three forms: dissolved in plasma (7–10%), bound to Hb as carbaminohemoglobin (20%), and as bicarbonate ions (70%). The carbonic anhydrase enzyme catalyzes the conversion of CO2 and water to carbonic acid, which dissociates into bicarbonate and hydrogen ions.
Carbonic Acid-Bicarbonate Buffer System: Maintains blood pH within a narrow range (7.35–7.45).
Neural Control of Ventilation
Control Centers
The medulla oblongata and pons in the brainstem regulate the basic rhythm and depth of breathing. Central and peripheral chemoreceptors monitor CO2, O2, and pH levels to adjust ventilation accordingly.
Central Chemoreceptors: Located in the medulla; respond to changes in CO2 and H+ in cerebrospinal fluid.
Peripheral Chemoreceptors: Located in carotid and aortic bodies; respond to changes in arterial PO2, PCO2, and pH.
Obstructive Lung Diseases
Overview
Obstructive lung diseases increase airway resistance and decrease the efficiency of expiration, leading to air trapping and reduced vital capacity.
Chronic Obstructive Pulmonary Disease (COPD): Includes emphysema, small airway disease, and chronic bronchitis; most commonly caused by smoking.
Asthma: Hyperresponsive airways with bronchoconstriction, inflammation, and mucus production.
Lung Cancer: Malignant tumors of the respiratory epithelium; smoking is the primary risk factor.
