 Back
BackChapter 22: The Respiratory System – Structure, Function, and Regulation
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
The Respiratory System
Overview and Major Functions
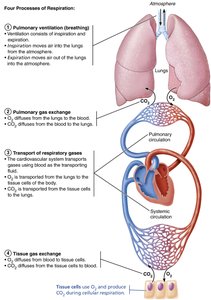
The respiratory system is essential for supplying the body with oxygen and removing carbon dioxide, a waste product of metabolism. It accomplishes this through a series of coordinated processes collectively known as respiration.
Pulmonary ventilation: Movement of air into and out of the lungs (breathing).
External respiration: Gas exchange between the lungs and the blood (pulmonary gas exchange).
Transport of respiratory gases: Movement of oxygen and carbon dioxide between the lungs and tissues via the blood.
Internal respiration: Gas exchange between systemic blood vessels and tissues (tissue gas exchange).
Organs and Passageways of the Respiratory System
Major Organs (in Descending Order)
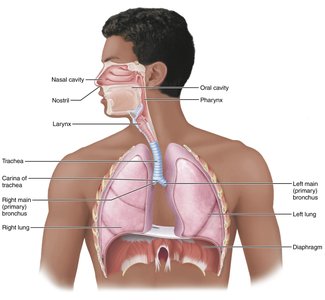
Nose
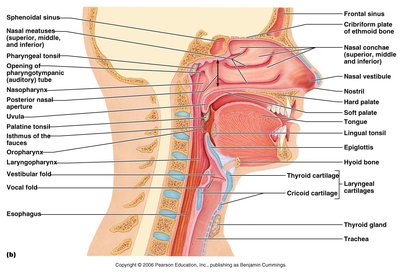
Nasal cavity/Paranasal sinuses
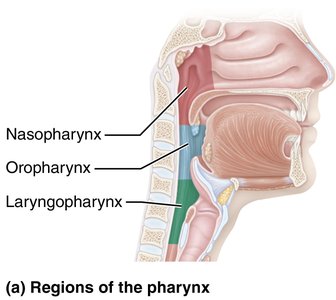
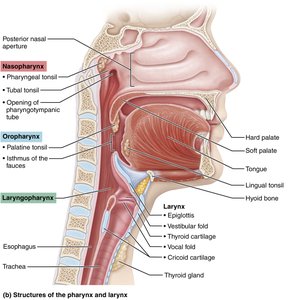
Pharynx (nasopharynx, oropharynx, laryngopharynx)
Larynx
Trachea
Bronchi and bronchial tree
Alveoli
Respiratory membrane
Upper and Lower Respiratory System
Structure | Description | Function |
|---|---|---|
Nose & Nasal Cavity | External structure supported by bone and cartilage; internal cavity divided by septum, lined with mucosa | Filters, warms, moistens air; resonance for speech; olfactory receptors |
Paranasal Sinuses | Air-filled cavities in cranial bones | Lighten skull; warm/moisten/filter air |
Pharynx | Muscular tube connecting nasal cavity/mouth to larynx/esophagus | Passageway for air/food; houses tonsils |
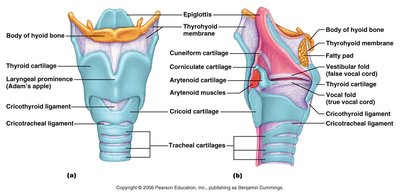
Larynx | Cartilaginous structure connecting pharynx to trachea | Air passageway; prevents food entry; voice production |
Trachea | Flexible tube with C-shaped cartilage rings | Air passageway; cleans, warms, moistens air |
Bronchial Tree | Branching system of bronchi/bronchioles | Air passageways; cleans, warms, moistens air |
Alveoli | Microscopic air sacs | Main sites of gas exchange; surfactant production |
Lungs | Paired organs with elastic connective tissue | House respiratory passages; allow passive recoil |
Pleurae | Serous membranes (parietal and visceral) | Produce lubricating fluid; compartmentalize lungs |



Conducting and Respiratory Zones
The respiratory system is divided into conducting and respiratory zones:
Conducting zone: Passageways that transport air to the respiratory zone (nose, nasal cavity, pharynx, larynx, trachea, bronchi, bronchioles).
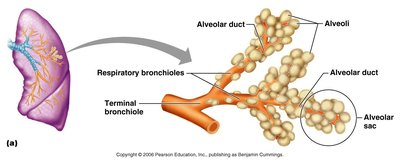
Respiratory zone: Site of gas exchange (respiratory bronchioles, alveolar ducts, alveoli).
Microscopic Structure and Gas Exchange
Respiratory Zone and Alveoli
The respiratory zone begins where terminal bronchioles feed into respiratory bronchioles, which lead to alveolar ducts and alveolar sacs. Alveoli are the primary sites of gas exchange, with approximately 300 million in the lungs, providing a large surface area.
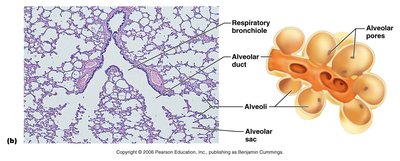
Respiratory Membrane
Composed of alveolar and capillary walls with fused basal laminas.
Type I alveolar cells: Simple squamous epithelium for gas diffusion.
Type II alveolar cells: Secrete surfactant to reduce surface tension.
Alveolar macrophages: Remove debris and pathogens.
Mechanics of Breathing
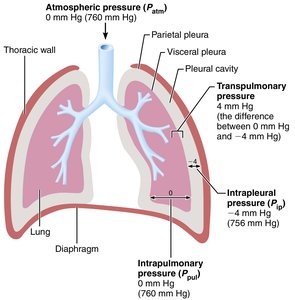
Pressure Relationships in the Thoracic Cavity
Atmospheric pressure (Patm): Pressure exerted by air around the body (760 mmHg at sea level).
Intrapulmonary pressure (Ppul): Pressure within alveoli; equalizes with atmospheric pressure during breathing cycles.
Intrapleural pressure (Pip): Pressure within pleural cavity; always negative relative to Patm and Ppul.
Transpulmonary pressure: Difference between Ppul and Pip; keeps lungs inflated.
Boyle’s Law and Pulmonary Ventilation
Boyle’s Law describes the inverse relationship between pressure and volume of a gas:
As thoracic volume increases, intrapulmonary pressure decreases, causing air to flow into the lungs (inspiration).
As thoracic volume decreases, intrapulmonary pressure increases, causing air to flow out (expiration).
Gas Exchange and Transport
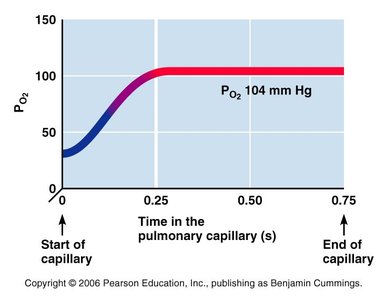
External Respiration (Pulmonary Gas Exchange)
Oxygen diffuses from alveoli (PO2 = 104 mmHg) into pulmonary capillaries (PO2 = 40 mmHg).
Carbon dioxide diffuses from blood (PCO2 = 45 mmHg) into alveoli (PCO2 = 40 mmHg).
CO2 is 20 times more soluble than O2, so it diffuses efficiently despite a smaller gradient.
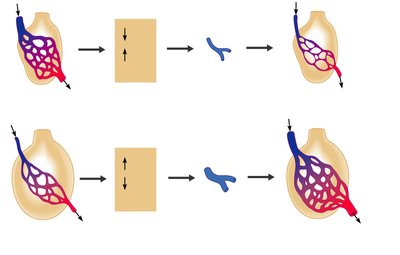
Ventilation-Perfusion Coupling
Efficient gas exchange requires matching of alveolar ventilation (airflow) and pulmonary perfusion (blood flow). Local changes in CO2 and O2 concentrations regulate bronchiolar and arteriolar diameter to optimize exchange.
Internal Respiration (Tissue Gas Exchange)
Oxygen diffuses from systemic capillaries into tissues (where PO2 is lower).
CO2 diffuses from tissues into blood (where PCO2 is lower).
Oxygen Transport
98.5% of O2 is carried bound to hemoglobin (Hb) as oxyhemoglobin (HbO2).
Each Hb molecule binds up to four O2 molecules.
O2 binding and release are influenced by PO2, temperature, pH, PCO2, and BPG.
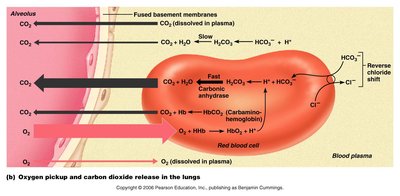
Carbon Dioxide Transport
7–10% dissolved in plasma
20% bound to Hb as carbaminohemoglobin
~70% as bicarbonate ion (HCO3–) in plasma
CO2 + H2O H2CO3 $\rightarrow$ H+ + HCO3–
The chloride shift maintains ionic balance as HCO3– exits RBCs and Cl– enters.
Control of Respiration
Neural Regulation
Medullary respiratory centers (VRG and DRG) set basic rhythm and integrate sensory input.
Pontine centers smooth transitions between inspiration and expiration.
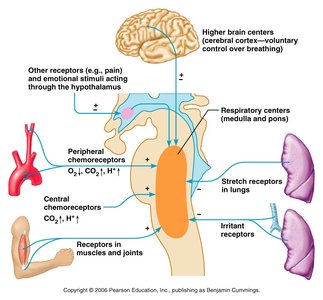
Chemical Factors
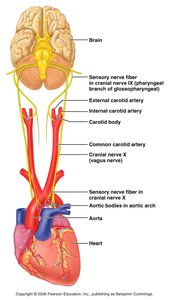
Central chemoreceptors (brainstem) and peripheral chemoreceptors (aortic arch, carotid arteries) monitor CO2, O2, and pH.
CO2 is the most potent stimulus for breathing; increased CO2 (hypercapnia) increases ventilation.
Low O2 (hypoxemia) stimulates breathing only when very low.
pH changes (acidosis/alkalosis) also affect respiratory rate.
Respiratory Pathophysiology
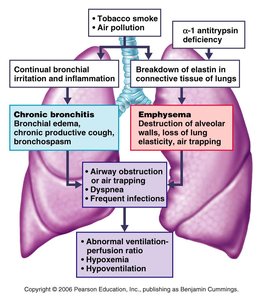
Chronic Obstructive Pulmonary Disease (COPD)
Includes chronic bronchitis and emphysema.
Characterized by airway obstruction, dyspnea, frequent infections, and abnormal ventilation-perfusion ratios.
Most common cause: smoking.
Asthma
Characterized by reversible airway inflammation, bronchospasm, and increased mucus production.
Triggered by immune responses and environmental factors.
Emphysema
Permanently enlarged alveoli and destruction of alveolar walls.
Loss of lung elasticity, air trapping, and increased work of breathing.
Chronic Bronchitis
Chronic inflammation and excessive mucus production in lower airways.
Obstructs airflow and increases risk of infection.
Tuberculosis
Infectious disease caused by Mycobacterium tuberculosis.
Symptoms: fever, night sweats, weight loss, cough.
Treatment: long-term antibiotics.
Lung Cancer
Leading cause of cancer death; strongly linked to smoking.
Types: squamous cell carcinoma, adenocarcinoma, small cell carcinoma.
