 Back
BackChapter 23: The Digestive System - Anatomy & Physiology II Study Notes
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
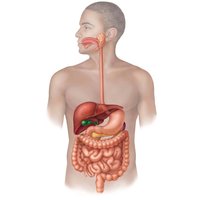
The Digestive System
Overview and Main Functions
The digestive system is responsible for the intake, breakdown, absorption, and elimination of food. It transforms food into nutrients that can be absorbed into the bloodstream and removes indigestible remains.
Ingestion: Eating and taking in food.
Mechanical and Chemical Breakdown: Food is broken down into smaller molecules by physical and enzymatic processes.
Absorption: Nutrient molecules are absorbed into the blood and lymphatic vessels.
Defecation: Elimination of indigestible substances as feces.
Components of the Digestive System
Alimentary Canal (GI Tract): Continuous muscular tube from mouth to anus. Includes mouth, pharynx, esophagus, stomach, small intestine, large intestine, and anus.
Accessory Digestive Organs: Teeth, tongue, gallbladder, salivary glands, liver, and pancreas. These organs produce secretions that aid digestion.
Digestive Processes
Six Essential Activities
Ingestion: Intake of food.
Propulsion: Movement of food through the GI tract, including swallowing and peristalsis.
Mechanical Breakdown: Chewing, mixing with saliva, churning in the stomach, and segmentation in the intestines.
Digestion: Enzymatic breakdown of complex molecules into simpler building blocks.
Absorption: Passage of digested fragments into blood or lymph.
Defecation: Elimination of indigestible substances.

Organization of the Digestive System
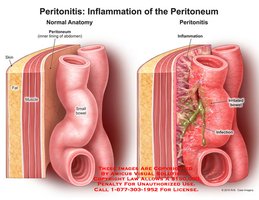
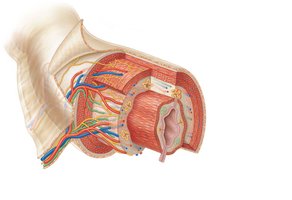
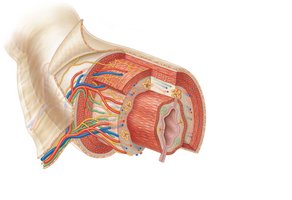
Peritoneum and Mesenteries
The peritoneum is a serous membrane lining the abdominal cavity.
Visceral Peritoneum: Covers external surfaces of digestive organs.
Parietal Peritoneum: Lines the body wall.
Peritoneal Cavity: Fluid-filled space between the two peritoneums, lubricating organs.
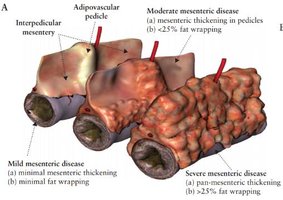
Mesentery: Double layer of peritoneum that supports organs, provides routes for vessels and nerves, and stores fat.
Intraperitoneal Organs: Located within the peritoneum.
Retroperitoneal Organs: Located outside or posterior to the peritoneum.

Clinical Note: Peritonitis
Peritonitis: Inflammation of the peritoneum, often caused by infection or injury. Can be life-threatening if widespread.
Treatment: Removal of debris and antibiotics.
Histology of the Alimentary Canal
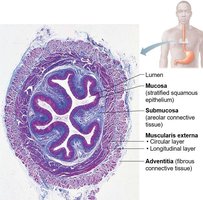
Four Basic Layers (Tunics)
Mucosa: Lines the lumen; secretes mucus, enzymes, and hormones; absorbs end products; protects against infection.
Epithelium: Simple columnar in most tract; stratified squamous in mouth, esophagus, anus.
Lamina Propria: Loose connective tissue with capillaries and lymphoid follicles (MALT).
Muscularis Mucosae: Smooth muscle for local movements.
Submucosa: Areolar connective tissue with blood vessels, lymphatics, and nerve plexus.
Muscularis Externa: Responsible for segmentation and peristalsis; inner circular and outer longitudinal layers; forms sphincters.
Serosa: Outermost layer; visceral peritoneum. In esophagus, replaced by adventitia (fibrous connective tissue).
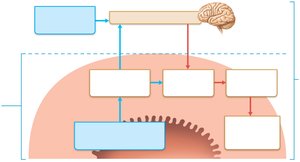
Enteric Nervous System
Intrinsic Nerve Plexuses
The GI tract has its own nervous system, the enteric nervous system ("gut brain"), which controls motility and secretions.
Submucosal Plexus: Regulates glands and smooth muscle in mucosa.
Myenteric Plexus: Controls GI tract motility.
Reflex Arcs
Short Reflexes: Mediated by enteric plexuses; respond to local stimuli.
Long Reflexes: Involve CNS; respond to internal and external stimuli.
Parasympathetic: Enhances digestion.
Sympathetic: Inhibits digestion.
Functional Anatomy of the Digestive System
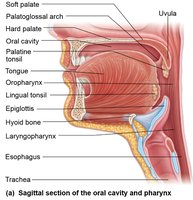
Mouth and Associated Organs
The mouth is the entry point for food, where mechanical and chemical digestion begins.
Boundaries: Lips, cheeks, palate, tongue.
Epithelium: Stratified squamous, keratinized in some areas for protection.

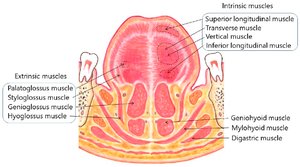
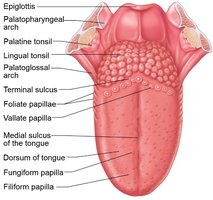
Tongue
The tongue is a muscular organ involved in food manipulation, taste, and speech.
Intrinsic Muscles: Change shape of tongue.
Extrinsic Muscles: Alter tongue position.
Papillae: Filiform (friction, no taste buds), fungiform (taste), vallate (taste), foliate (taste).
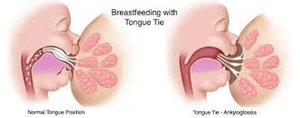
Clinical Note: Ankyloglossia
Ankyloglossia: "Tongue-tied" condition due to short lingual frenulum; affects speech and feeding.
Treatment: Surgical snipping of frenulum.
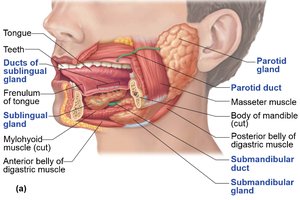
Salivary Glands
Salivary glands produce saliva, which cleanses the mouth, dissolves food, moistens food, and begins starch digestion.
Major Glands: Parotid, submandibular, sublingual.
Secretory Cells: Serous (watery, enzymes), mucous (mucus).
Saliva Composition: Water, electrolytes, amylase, lipase, mucin, lysozyme, IgA.
Clinical Note: Xerostomia
Xerostomia: Dry mouth due to reduced saliva; can cause oral infections and difficulty swallowing.

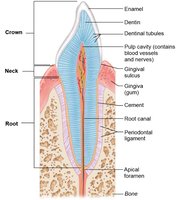
Teeth
Teeth are essential for mastication (chewing), breaking food into smaller fragments.
Types: Incisors (cutting), canines (tearing), premolars (grinding), molars (grinding).
Structure: Crown (enamel), neck, root (cement, periodontal ligament, dentin, pulp cavity).
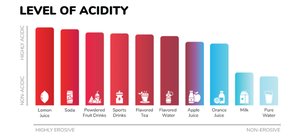
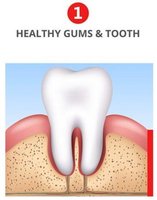
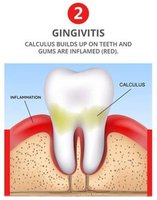
Clinical Note: Dental Caries and Periodontal Disease
Dental Caries: Cavities from bacterial action; prevention by brushing and flossing.
Gingivitis: Inflammation of gums due to plaque and calculus.
Periodontitis: Advanced gum disease; can lead to tooth loss and systemic effects.

The Pharynx and Esophagus
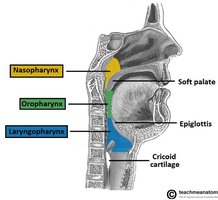
Pharynx
The pharynx is a muscular tube that allows passage of food, fluids, and air.
Regions: Oropharynx, laryngopharynx.
Epithelium: Stratified squamous with mucus glands.
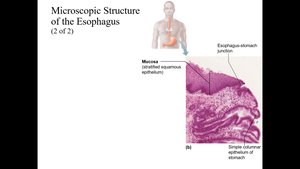
Esophagus
The esophagus is a muscular tube connecting the pharynx to the stomach.
Layers: Mucosa (stratified squamous), submucosa, muscularis externa, adventitia.
Gastroesophageal Sphincter: Prevents reflux of stomach contents.
Clinical Note: Heartburn and GERD
Heartburn: Stomach acid regurgitation; can lead to GERD, esophagitis, ulcers, or cancer.

Digestive Processes: Mouth to Esophagus
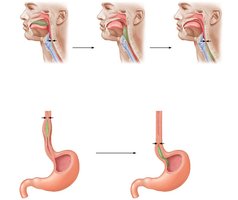
Swallowing and Peristalsis
Swallowing moves food from mouth to esophagus, followed by peristalsis to the stomach.
Buccal Phase: Voluntary; tongue pushes bolus into oropharynx.
Pharyngeal-Esophageal Phase: Involuntary; soft palate closes nasopharynx, epiglottis closes trachea, peristalsis moves food down esophagus.
The Stomach
Anatomy and Function
The stomach is a muscular organ that stores food and begins protein digestion.
Regions: Cardia, fundus, body, pyloric part.
Rugae: Folds in mucosa when empty.
Pyloric Sphincter: Controls emptying into duodenum.
Microscopic Anatomy
Muscularis Externa: Three layers: longitudinal, circular, oblique.
Mucosa: Secretes alkaline mucus; contains gastric pits with specialized cells:
Mucous Neck Cells: Secrete mucus.
Parietal Cells: Secrete HCl and intrinsic factor.
Chief Cells: Secrete pepsinogen.
Enteroendocrine Cells: Secrete hormones.


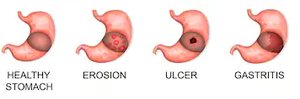
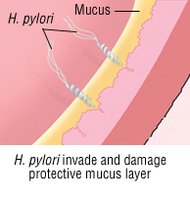
Clinical Note: Gastritis and Ulcers
Gastritis: Inflammation of stomach mucosa.
Peptic Ulcers: Erosions caused by Helicobacter pylori or NSAIDs.
Digestive Processes in the Stomach
Breakdown of Food: Denaturation of proteins by HCl, enzymatic digestion by pepsin.
Intrinsic Factor: Essential for vitamin B12 absorption.
Regulation: Neural (vagus, sympathetic) and hormonal (gastrin) mechanisms.
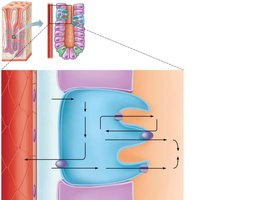
Mechanism of HCl Secretion
Parietal cells secrete HCl via the following process:
CO2 and H2O combine to form H2CO3 (carbonic acid) via carbonic anhydrase.
H2CO3 dissociates into H+ and HCO3-.
H+ is pumped into the lumen in exchange for K+ (via H+-K+ ATPase).
Cl- diffuses into the lumen and combines with H+ to form HCl.
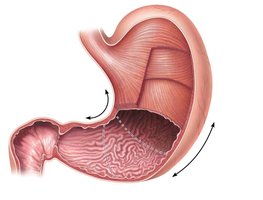
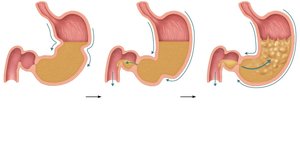
Peristaltic Waves in the Stomach
Propulsion: Peristaltic waves move food toward pylorus.
Grinding: Vigorous mixing at pyloric end.
Retropulsion: Most contents forced backward into stomach.
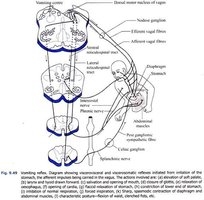
Clinical Note: Vomiting (Emesis)
Causes: Extreme stretching, irritants, toxins.
Risks: Dehydration, electrolyte, and acid-base imbalances.
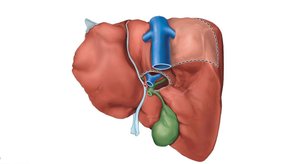
Liver, Gallbladder, and Pancreas
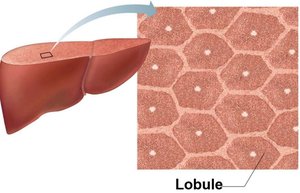
Liver
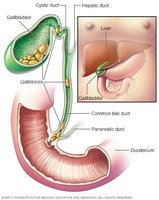
The liver is the largest gland, producing bile for fat emulsification.
Lobes: Right, left, caudate, quadrate.
Bile Ducts: Common hepatic, cystic, and bile duct.
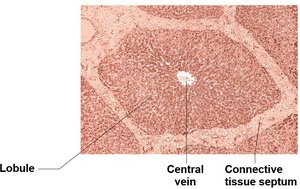
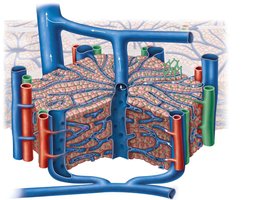
Microscopic Anatomy
Lobules: Hexagonal units with plates of hepatocytes.
Portal Triad: Branch of hepatic artery, portal vein, and bile duct.
Sinusoids: Leaky capillaries; stellate macrophages remove debris.
Bile and Enterohepatic Circulation
Bile: Contains bile salts (fat emulsification), bilirubin (pigment), cholesterol, phospholipids, electrolytes.
Enterohepatic Circulation: Bile salts are recycled from intestine to liver.
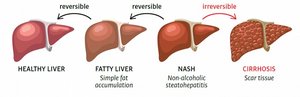
Clinical Note: Liver Disease
Hepatitis: Viral infection, drug toxicity.
Cirrhosis: Chronic inflammation, fibrosis, portal hypertension.
Gallbladder
Function: Stores and concentrates bile.
Clinical Note: Gallstones (biliary calculi) can block bile flow, cause pain, and jaundice.
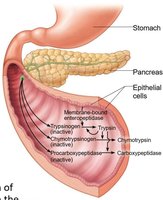
Pancreas
Exocrine Function: Produces pancreatic juice (enzymes, bicarbonate).
Endocrine Function: Secretes insulin and glucagon.
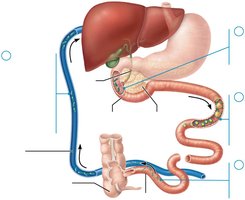
The Small Intestine
Anatomy and Modifications
The small intestine is the major organ of digestion and absorption.
Subdivisions: Duodenum, jejunum, ileum.
Structural Modifications: Circular folds, villi, microvilli (brush border) increase surface area for absorption.
Clinical Note: Chemotherapy Effects
Targets rapidly dividing cells, including GI epithelium, causing nausea, vomiting, diarrhea.
The Large Intestine
Anatomy and Features
The large intestine absorbs water and electrolytes, forms feces, and houses bacterial flora.
Features: Teniae coli, haustra, epiploic appendages.
Subdivisions: Cecum, appendix, colon (ascending, transverse, descending, sigmoid), rectum, anal canal.
Clinical Note: Appendicitis
Acute inflammation of appendix; can cause peritonitis if ruptured.
Bacterial Flora
Fermentation of indigestible carbohydrates, vitamin synthesis, immune protection.
Clinical Note: Antibiotic-Associated Diarrhea
Clostridium difficile infection can cause severe colitis.
Digestive Processes in the Large Intestine
Propulsion of feces, absorption of water and electrolytes, defecation.
Clinical Note: Diverticulosis and IBS
Diverticulosis: Herniations in colon wall; can become inflamed (diverticulitis).
Irritable Bowel Syndrome: Functional disorder with abdominal pain, stool changes, and stress-related symptoms.
Clinical Note: Diarrhea and Constipation
Diarrhea: Rapid transit prevents water absorption; can cause dehydration.
Constipation: Prolonged transit increases water absorption; stool becomes hard.
Mechanisms of Digestion and Absorption
Enzymatic Hydrolysis
Digestion breaks down macromolecules into monomers via hydrolysis, allowing absorption across the intestinal wall.
Absorption Mechanisms
Substances pass through epithelial cells via apical and basolateral membranes.
Lipid molecules are absorbed passively; polar molecules require active transport.
Carbohydrate Digestion and Absorption
Starch and disaccharides are broken down by amylase and brush border enzymes into monosaccharides.
Glucose and galactose are absorbed via Na+-cotransport; fructose via facilitated diffusion.
Clinical Note: Lactose Intolerance
Deficiency of lactase leads to undigested lactose, causing diarrhea, bloating, and cramping.
Protein Digestion and Absorption
Proteins are broken down by pepsin, pancreatic enzymes, and brush border enzymes into amino acids.
Amino acids are absorbed via Na+-cotransport.
Lipid Digestion and Absorption
Emulsification by bile salts, digestion by pancreatic lipases, micelle formation, diffusion, chylomicron formation, and transport via lymph.
Nucleic Acid Digestion and Absorption
Pancreatic nucleases and brush border enzymes break down nucleic acids; absorbed via active transport.
Absorption of Vitamins, Electrolytes, and Water
Fat-soluble vitamins (A, D, E, K) absorbed with micelles; water-soluble vitamins by diffusion or transporters.
Electrolytes actively transported; water absorbed by osmosis.
Clinical Note: Malabsorption and Celiac Disease
Malabsorption can result from impaired delivery of bile or pancreatic juice, or damaged intestinal mucosa.
Celiac disease is an immune reaction to gluten, damaging villi and brush border.
Summary Table: Digestive System Organs and Functions
Organ | Main Function |
|---|---|
Mouth | Ingestion, mechanical breakdown, starch digestion |
Pharynx | Passage of food, fluids, air |
Esophagus | Propulsion of food to stomach |
Stomach | Protein digestion, food storage, mechanical breakdown |
Small Intestine | Digestion, absorption of nutrients |
Large Intestine | Absorption of water/electrolytes, feces formation |
Liver | Bile production, metabolism, detoxification |
Gallbladder | Bile storage and concentration |
Pancreas | Enzyme and bicarbonate secretion, hormone production |
Key Equations
Mechanism of HCl Secretion
Na+-K+ ATPase (Active Transport)
Additional info:
Clinical notes and disease mechanisms were expanded for academic completeness.
Tables and diagrams were recreated for clarity and exam preparation.
