 Back
BackCranial Nerves: Structure, Function, and Clinical Relevance
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Cranial Nerves: Structure, Function, and Clinical Relevance
Introduction to the Peripheral Nervous System and Cranial Nerves
The peripheral nervous system (PNS) gathers input from sensory receptors and sends motor output to effectors, communicating with the central nervous system (CNS). Cranial nerves are a key component of the PNS, responsible for sensory and motor innervation of the head and neck, and some structures in the thorax and abdomen.
Overview of Cranial Nerves
There are 12 pairs of cranial nerves, each with specific sensory, motor, or mixed functions. They are numbered I through XII from rostral (front) to caudal (back). Most cranial nerves attach to the brainstem, except for the first two pairs, which attach to the forebrain. The mnemonic "Some say marry money, but my brother believes big brains matter more" helps remember their primary functions (sensory, motor, or both).
Cranial Nerve I: Olfactory Nerve
Structure and Function
Origin: Olfactory sensory neurons in the nasal cavity.
Pathway: Fibers pass through the cribriform plate of the ethmoid bone to the olfactory bulbs, then to the primary olfactory cortex.
Function: Purely sensory; responsible for the sense of smell.
Clinical Testing: Identification of aromatic substances (e.g., oil of cloves, vanilla).
Homeostatic Imbalance: Damage can cause anosmia (loss of smell).
Cranial Nerve II: Optic Nerve
Structure and Function
Origin: Retina of the eye.
Pathway: Passes through the optic canal, forms the optic chiasma, continues as optic tracts to the thalamus, and then to the occipital cortex.
Function: Purely sensory; responsible for vision.
Clinical Testing: Visual field tests, eye chart, ophthalmoscopic examination.
Homeostatic Imbalance: Damage can cause anopsias (visual field defects) or blindness.
Cranial Nerve III: Oculomotor Nerve
Structure and Function
Origin: Ventral midbrain.
Pathway: Passes through the superior orbital fissure to the eye.
Function: Chiefly motor; controls most eye movements, pupil constriction, and lens shape.
Clinical Testing: Pupil response to light, eye movement tracking.
Homeostatic Imbalance: Paralysis leads to double vision, drooping eyelid (ptosis), and difficulty focusing.
Cranial Nerve IV: Trochlear Nerve
Structure and Function
Origin: Dorsal midbrain.
Pathway: Enters orbit via superior orbital fissure.
Function: Motor; innervates the superior oblique muscle of the eye.
Clinical Testing: Eye movement tests (with CN III).
Homeostatic Imbalance: Damage causes double vision and impaired downward/lateral movement.
Cranial Nerve V: Trigeminal Nerve
Structure and Function
Origin: Pons.
Divisions: Ophthalmic (V1), Maxillary (V2), Mandibular (V3).
Function: Mixed; sensory for face, motor for mastication.


Division | Origin & Course | Function | Clinical Testing |
|---|---|---|---|
Ophthalmic (V1) | Face to pons via superior orbital fissure | Sensory from scalp, upper eyelid, nose, cornea | Corneal reflex (blinking) |
Maxillary (V2) | Face to pons via foramen rotundum | Sensory from cheek, upper lip, lower eyelid | Pain, touch, temperature tests |
Mandibular (V3) | Face to pons via foramen ovale | Sensory from chin, lower teeth; motor to chewing muscles | Jaw movement, resistance tests |
Homeostatic Imbalance: Trigeminal neuralgia causes severe facial pain, often triggered by mild stimuli.
Cranial Nerve VI: Abducens Nerve
Structure and Function
Origin: Inferior pons.
Pathway: Enters orbit via superior orbital fissure.
Function: Motor; innervates lateral rectus muscle (eye abduction).
Clinical Testing: Eye movement tests (with CN III).
Homeostatic Imbalance: Paralysis causes inability to move eye laterally; eye may turn medially at rest.
Cranial Nerve VII: Facial Nerve
Structure and Function
Origin: Pons.
Pathway: Internal acoustic meatus, stylomastoid foramen to face.
Function: Mixed; motor to facial expression muscles, parasympathetic to glands, sensory for taste (anterior 2/3 of tongue).
Clinical Testing: Taste tests, facial movement symmetry, tear production.
Homeostatic Imbalance: Bell's palsy causes facial paralysis and loss of taste; often recovers with treatment.
Cranial Nerve VIII: Vestibulocochlear Nerve
Structure and Function
Origin: Inner ear (cochlea and vestibule).
Pathway: Internal acoustic meatus to brainstem.
Function: Mostly sensory; hearing (cochlear) and equilibrium (vestibular).
Clinical Testing: Hearing tests (tuning fork), balance assessment.
Homeostatic Imbalance: Damage causes deafness, dizziness, loss of balance, nausea.
Cranial Nerve IX: Glossopharyngeal Nerve
Structure and Function
Origin: Medulla.
Pathway: Exits skull via jugular foramen to throat.
Function: Mixed; motor to pharynx (swallowing), parasympathetic to parotid gland, sensory for taste (posterior 1/3 of tongue), and baro/chemoreceptor input.
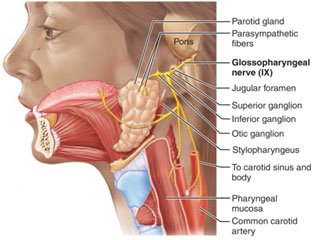
Clinical Testing: Gag reflex, swallowing, taste on posterior tongue.
Homeostatic Imbalance: Damage impairs swallowing and taste.
Cranial Nerve X: Vagus Nerve
Structure and Function
Origin: Medulla.
Pathway: Exits skull via jugular foramen, extends to thorax and abdomen.
Function: Mixed; parasympathetic control of heart, lungs, digestive tract; sensory from viscera, baro/chemoreceptors, taste buds.
Clinical Testing: Same as glossopharyngeal nerve (IX).
Homeostatic Imbalance: Paralysis can cause hoarseness, swallowing difficulty, and impaired organ function.
Cranial Nerve XI: Accessory Nerve
Structure and Function
Origin: Rootlets from C1–C5 spinal cord segments.
Pathway: Enters skull via foramen magnum, exits via jugular foramen.
Function: Primarily motor; innervates sternocleidomastoid and trapezius muscles (head and neck movement).
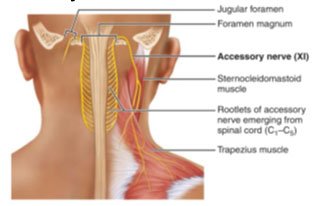
Clinical Testing: Shoulder shrug and head rotation against resistance.
Homeostatic Imbalance: Injury causes weakness in head rotation and shoulder elevation.
Cranial Nerve XII: Hypoglossal Nerve
Structure and Function
Origin: Medulla.
Pathway: Exits skull via hypoglossal canal to tongue.
Function: Primarily motor; controls tongue movements for speech, chewing, and swallowing.
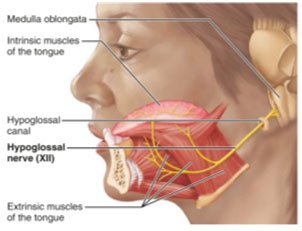
Clinical Testing: Tongue protrusion and retraction; deviation indicates nerve damage.
Homeostatic Imbalance: Damage causes speech and swallowing difficulties; tongue may deviate toward affected side.
Summary Table: Cranial Nerves Overview
Number | Name | Type | Main Function |
|---|---|---|---|
I | Olfactory | Sensory | Smell |
II | Optic | Sensory | Vision |
III | Oculomotor | Motor | Eye movement, pupil constriction |
IV | Trochlear | Motor | Eye movement (superior oblique) |
V | Trigeminal | Both | Facial sensation, mastication |
VI | Abducens | Motor | Eye movement (lateral rectus) |
VII | Facial | Both | Facial expression, taste, glands |
VIII | Vestibulocochlear | Sensory | Hearing, balance |
IX | Glossopharyngeal | Both | Taste, swallowing, salivation |
X | Vagus | Both | Viscera control, taste, sensory |
XI | Accessory | Motor | Head and neck movement |
XII | Hypoglossal | Motor | Tongue movement |
Additional info:
The cranial nerves are essential for sensory and motor functions of the head and neck, and some also influence thoracic and abdominal organs.
Mnemonic devices are commonly used to remember the order and function of cranial nerves.
