 Back
BackDevelopment of the Respiratory System: Embryology and Clinical Correlates
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Development of the Respiratory System
Introduction
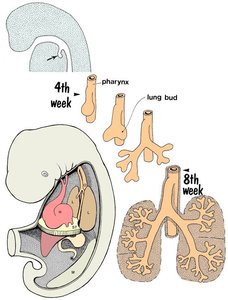
The respiratory system, comprising the larynx, trachea, bronchi, and lungs, begins its development during the fourth week of embryogenesis. This process involves complex interactions between endodermal and mesodermal tissues, resulting in the formation of functional respiratory structures essential for postnatal life.
Development of the Larynx
Embryological Origin and Morphogenesis
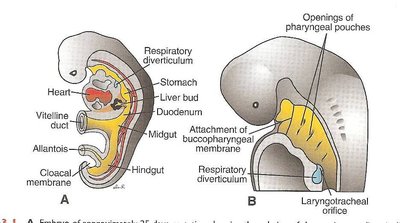
Laryngotracheal Groove: The respiratory primordium appears as a median outgrowth from the ventral wall of the primordial pharynx, forming the laryngotracheal groove.
Laryngotracheal Diverticulum: This groove deepens to form the laryngotracheal diverticulum, which elongates into the laryngotracheal tube.
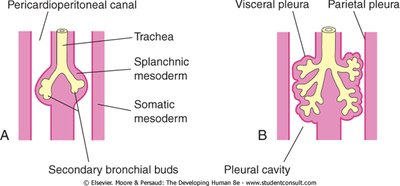
Germ Layer Contributions: The endoderm gives rise to the epithelium and glands of the larynx, while the splanchnic mesoderm forms the cartilages, smooth muscles, and connective tissues.
Laryngeal Cartilages and Muscles: These structures are derived from the 4th and 6th pairs of pharyngeal arches.
Epiglottis: Develops from the caudal part of the hypopharyngeal eminence.
Development of the Trachea
Separation from the Foregut and Tissue Differentiation
Tracheoesophageal Septum: The tracheoesophageal septum divides the cranial part of the foregut into the laryngotracheal tube (ventral) and the esophagus (dorsal).
Endodermal Lining: Forms the epithelium and glands of the trachea.
Splanchnic Mesenchyme: Gives rise to cartilage, connective tissue, and smooth muscle of the trachea.
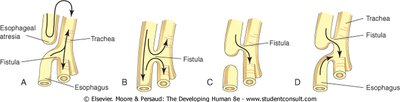
Tracheoesophageal Fistula (TEF)
Definition: An abnormal communication between the trachea and esophagus, usually due to incomplete division of the foregut during the fourth week.
Clinical Association: TEF is a component of the VACTERL association (Vertebral anomalies, Anal atresia, Cardiac defects, TEF, Esophageal atresia, Renal anomalies, Limb defects).
Development of Bronchi and Lungs
Branching Morphogenesis and Stages of Lung Development
Bronchial Buds: The laryngotracheal tube gives rise to right and left primary bronchial buds, which further subdivide into secondary and segmental bronchi.
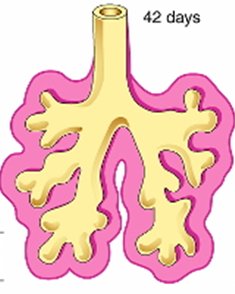
Branching: By the 24th week, about 17 orders of branches are formed, including respiratory bronchioles. An additional 7 generations of branches form after birth, up to 8 years of age.
Stages of Lung Development
Pseudoglandular Stage (6–16 weeks): Major elements of the lung are formed, but no respiratory bronchioles are present.
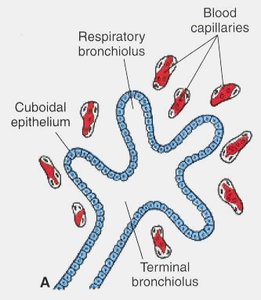
Canalicular Stage (16–26 weeks): Terminal bronchioles divide into respiratory bronchioles, which further divide into alveolar ducts. Respiration becomes possible at the end of this period as terminal saccules (primordial alveoli) develop and lung tissue becomes well vascularized.
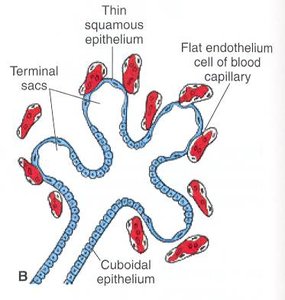
Terminal Sac Stage (26 weeks to birth): More terminal sacs form, lined by squamous epithelium. There is intimate contact between epithelial and endothelial cells. Surfactant secretion by alveolar type II cells begins by 20 weeks, reducing surface tension and facilitating postnatal respiration.
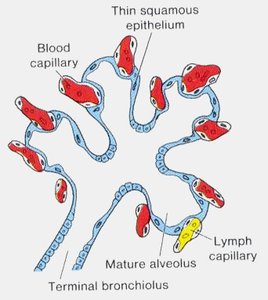
Alveolar Stage (32 weeks to after birth): Primitive alveoli with well-developed epithelial–endothelial capillary contacts (blood–air barrier) are present. Mature alveoli continue to form after birth as the lungs expand, with alveolar formation continuing up to 8–10 years of age.
Factors Influencing Normal Lung Development
Thoracic Space: Adequate space is necessary for lung growth.
Fetal Breathing Movements: Stimulate lung development.
Amniotic Fluid Volume: Oligohydramnios (insufficient amniotic fluid) can lead to pulmonary hypoplasia.
Congenital Diaphragmatic Hernia: Reduces thoracic space, impeding normal lung development.
Clinical Correlates and Congenital Anomalies
Lung Agenesis and Hypoplasia
Agenesis: Failure of bronchial buds to develop. Unilateral pulmonary agenesis is compatible with life, but the heart and mediastinal structures shift to the affected side, and the existing lung becomes hyperexpanded.
Lung Hypoplasia: Underdevelopment of the lungs, often associated with congenital diaphragmatic hernia or oligohydramnios.
Respiratory Distress Syndrome (RDS)
Hyaline Membrane Disease (HMD): Caused by surfactant deficiency, leading to underinflated lungs and alveoli filled with proteinaceous fluid resembling a hyaline membrane. Prolonged intrauterine asphyxia can cause irreversible changes in type II alveolar cells.
Congenital Lung Cysts
Definition: Cysts filled with fluid or air, formed by dilation of terminal bronchi due to disturbances in bronchial development during late fetal life.
Lobe of Azygos Vein and Accessory Lung
Lobe of Azygos Vein: An anatomical variant appearing in the right lung, visible on chest X-ray.
Accessory Lung: Rare, extra lung tissue separated from the main lungs.

Summary Table: Stages of Lung Development
Stage | Time Frame | Main Features |
|---|---|---|
Pseudoglandular | 6–16 weeks | Formation of major airways; no respiratory bronchioles |
Canalicular | 16–26 weeks | Formation of respiratory bronchioles and alveolar ducts; vascularization increases |
Terminal Sac | 26 weeks–birth | Formation of terminal sacs (primitive alveoli); surfactant production begins |
Alveolar | 32 weeks–8 years | Maturation and multiplication of alveoli; establishment of blood–air barrier |
Key Points
Respiratory system development begins in the 4th week from the laryngotracheal tube, a median outgrowth of the foregut.
Separation from the foregut is achieved by the tracheoesophageal septum.
Endoderm forms the epithelium and glands; splanchnic mesenchyme forms connective tissue, cartilage, muscle, blood, and lymphatic vessels.
Surfactant secretion by type II alveolar cells begins by 20 weeks gestation.
References: 1. Mark G. Torchia, T. V. N. Persaud (2024). The Developing Human. Clinically Oriented Embryology. 12th Edition. 2. T.W. Sadler (2018). Langman’s Medical Embryology. 14th Edition. Lippincott Williams & Wilkins.
