 Back
BackNutrients Important for Bone Health: Structure, Function, and Clinical Considerations
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Bone Structure and Function
The Importance of the Skeletal System
The skeletal system is essential for movement, structural support, and protection of internal organs. It also plays a critical role in hematopoiesis (blood cell formation) and mineral storage.
Movement: Bones and connective tissues (cartilage, tendons, ligaments) enable a wide range of movements.
Support and Protection: The skeleton provides a rigid framework for the body and shields vital organs.
Hematopoiesis: Red and white blood cells and platelets are produced in the bone marrow.
Mineral Storage: Bones act as reservoirs for calcium, phosphorus, and magnesium.

Bone Anatomy and Structure
The human skeleton consists of 206 bones, divided into the axial and appendicular skeletons. Bones are classified by shape and internal structure.
Axial Skeleton: Includes the skull, vertebral column, and rib cage (80 bones).
Appendicular Skeleton: Includes the shoulder girdle, pelvic girdle, and limbs (126 bones).
Bone Types: Long, short, flat, and irregular bones.
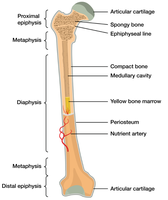
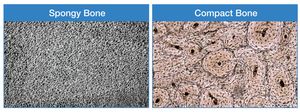
Bone Tissue Types
Bones are composed of inorganic (mineralized matrix, mainly hydroxyapatite) and organic materials, organized into two main tissue types:
Trabecular (Spongy) Bone: Porous, found at the ends of long bones and inside vertebrae.
Cortical (Compact) Bone: Dense, forms the outer layer of bones.
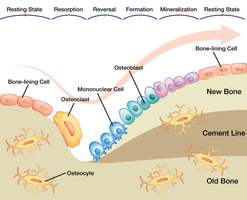
Bone Cells and Remodeling
Bone is a dynamic tissue, constantly remodeled through the coordinated actions of specialized cells:
Osteoblasts: Build new bone tissue.
Osteoclasts: Break down bone tissue (bone resorption).
Osteocytes: Mature bone cells that maintain bone matrix.
Bone remodeling involves resorption (osteoclasts dissolve bone matrix) followed by formation (osteoblasts lay down new bone). This process adapts bone to mechanical stress and repairs microdamage.
Micronutrients Essential for Bone Health
Calcium
Calcium is the most abundant mineral in the body and is vital for bone and tooth formation, nerve transmission, muscle contraction, and blood clotting.
Functions: Bone structure, nerve impulse transmission, muscle contraction, activation of clotting factors, insulin release, and energy for muscle contraction.
Sources: Dairy products, fortified foods, tofu, leafy greens.
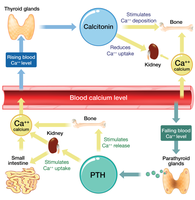
Calcium Homeostasis
Blood calcium levels are tightly regulated by three hormones:
Parathyroid Hormone (PTH): Increases blood calcium by stimulating bone resorption, kidney reabsorption, and intestinal absorption (with vitamin D).
Calcitriol (active vitamin D): Enhances intestinal absorption of calcium.
Calcitonin: Lowers blood calcium by inhibiting bone resorption and increasing renal excretion.
Vitamin D
Vitamin D is a fat-soluble vitamin essential for calcium absorption and bone health. It is synthesized in the skin upon exposure to sunlight and activated in the liver and kidneys to form calcitriol.
Functions: Promotes calcium absorption, maintains bone mineralization, supports immune function.
Deficiency Diseases: Nutritional rickets (children), osteomalacia (adults), increased risk of osteoporosis.
Sources: Sunlight, fatty fish, fortified foods.

Other Essential Micronutrients
Phosphorus: Second most abundant mineral in the body, mostly in bones. Found in many foods, especially processed foods.
Magnesium: Important for bone structure, ATP reactions, nerve conduction, and muscle contraction. Found in green leafy vegetables, fish, dairy, meats, whole grains, nuts, and hard water.
Fluoride: Strengthens bones and teeth, prevents tooth decay. Main source is fluoridated water.
Vitamin K: Acts as a coenzyme for proteins involved in bone metabolism and blood clotting. Found in green vegetables like broccoli, kale, and spinach.

Osteoporosis: Pathophysiology and Risk Factors
Definition and Types
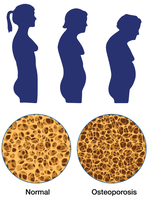
Osteoporosis is a disease characterized by excessive bone loss, leading to fragile bones and increased fracture risk.
Type 1 (Postmenopausal): Rapid bone loss due to decreased estrogen, common in women 50–70 years old.
Type 2 (Senile): Occurs after age 70, affects both sexes but more common in women, associated with hip and spine fractures.

Bone Mineral Density (BMD) and Diagnosis
Bone mineral density (BMD) is a measure of the amount of calcified tissue in bone and is used to assess fracture risk. The gold standard for measuring BMD is dual-energy X-ray absorptiometry (DEXA).
Peak Bone Mass: The highest amount of bone tissue achieved, usually in early adulthood.
Osteopenia: Lower than normal BMD, but not low enough to be classified as osteoporosis.
Risk Factors for Osteoporosis
Nonmodifiable: Age over 40, female sex, small frame, White or Asian ethnicity, low estrogen, family history, certain diseases and medications.
Modifiable: Physical inactivity, low body weight, smoking, excessive alcohol or caffeine, poor nutrition (especially low calcium and vitamin D), inadequate protein intake.
Osteoporosis Prevention and Treatment
Primary Prevention
Building peak bone mass during youth is critical. Prevention strategies include:
Adequate intake of calcium and vitamins A, C, D, E, and K
Regular weight-bearing exercise (e.g., walking, running, resistance training)
Fall prevention (home safety, vision and balance checks)
Secondary Prevention and Treatment
Address underlying diseases or medications that contribute to bone loss
Pharmacotherapy (medications to slow bone loss or increase bone formation)
Calcium Deficiency, Supplementation, and Dietary Choices
Groups at Risk for Calcium Inadequacy
Adolescents (especially teens with low dairy intake)
Women with amenorrhea or postmenopausal women (due to low estrogen)
Older adults (reduced calcium absorption)
Lactose-intolerant individuals and vegans (avoidance of dairy)
Calcium Supplementation
Common forms: calcium carbonate, citrate, lactate, phosphate
Supplements should be taken with vitamin D for optimal benefit
Split doses (≤500 mg at a time) improve absorption
Some natural-source supplements may contain lead
Dietary Considerations
Best calcium sources are dietary (dairy, fortified foods, leafy greens)
Excessive calcium can impair absorption of iron and zinc
High phosphate intake (e.g., from soda) can decrease bone health
Lactose-free diets may increase risk of inadequate bone mineralization
Summary Table: Key Micronutrients for Bone Health
Nutrient | Main Function | Sources | Deficiency Effects |
|---|---|---|---|
Calcium | Bone structure, muscle contraction, nerve transmission, clotting | Dairy, fortified foods, leafy greens | Osteopenia, osteoporosis, muscle cramps |
Vitamin D | Calcium absorption, bone mineralization | Sunlight, fatty fish, fortified foods | Rickets, osteomalacia, osteoporosis |
Phosphorus | Bone mineralization, energy metabolism | Meat, dairy, processed foods | Bone pain, muscle weakness (rare) |
Magnesium | Bone structure, enzyme function | Leafy greens, nuts, whole grains | Muscle cramps, osteoporosis risk |
Fluoride | Tooth and bone strength | Fluoridated water | Dental caries, weak bones |
Vitamin K | Bone protein modification, clotting | Green vegetables | Impaired bone health, bleeding |
