 Back
BackRespiratory Physiology: Mechanisms and Control of Breathing
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Respiratory Physiology
Overview of Respiration
Respiration is a vital process that ensures the delivery of oxygen to body tissues and the removal of carbon dioxide, a metabolic waste product. It involves several interconnected events: pulmonary ventilation, external respiration, gas transport, and internal respiration. Cellular respiration, which occurs in the mitochondria, uses oxygen to produce ATP, the energy currency of the cell.
Pulmonary ventilation (breathing): Movement of air into and out of the lungs.
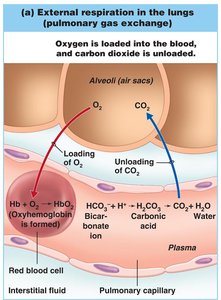
External respiration: Gas exchange between alveoli and blood.
Gas transport: Movement of gases in the blood between lungs and tissues.
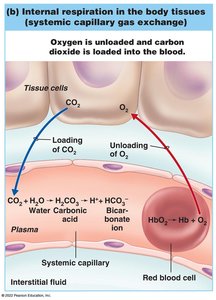
Internal respiration: Gas exchange between blood and tissue cells.
Cellular respiration: Utilization of oxygen by cells to produce ATP and carbon dioxide.

Mechanics of Breathing
Pulmonary Ventilation: Inspiration and Expiration
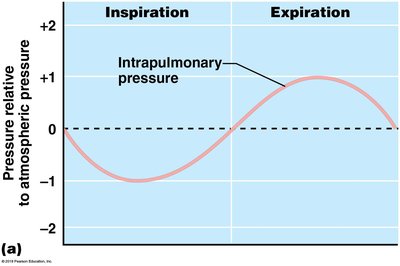
Breathing is driven by pressure changes in the thoracic cavity, which are created by the contraction and relaxation of respiratory muscles. According to Boyle’s Law, pressure and volume are inversely related: as thoracic volume increases, pressure decreases, and vice versa.
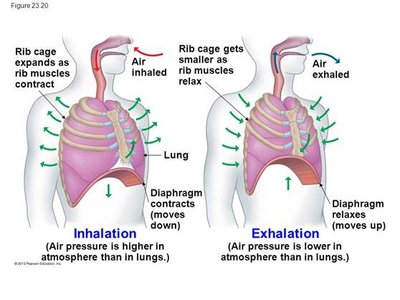
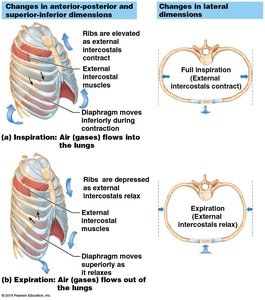
Inspiration: Diaphragm contracts and moves downward; external intercostal muscles contract, lifting the rib cage up and out. Thoracic volume increases, intrapulmonary pressure drops below atmospheric pressure, and air flows into the lungs.
Expiration: Diaphragm and external intercostals relax, thoracic volume decreases, intrapulmonary pressure rises above atmospheric pressure, and air is expelled from the lungs.
Rib Movements in Breathing
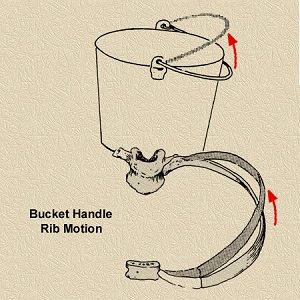
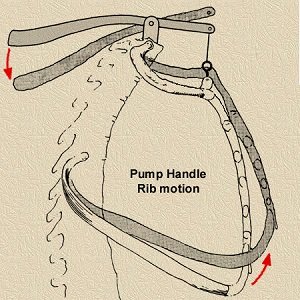
The rib cage expands and contracts in two main ways to facilitate breathing:
Bucket handle motion: Ribs move upward and outward, increasing the lateral dimension of the thoracic cavity.
Pump handle motion: Ribs move upward and forward, increasing the anterior-posterior dimension.
Muscle Actions During Breathing
Inhalation and exhalation involve coordinated actions of the diaphragm and intercostal muscles. During forced exhalation, abdominal muscles contract to push the diaphragm further upward.
Antagonistic Muscle Groups
Muscles can only contract to produce movement in one direction. Opposing muscle groups (antagonists) are required for movements in both directions, such as inspiration and expiration.
Intrapleural Pressure and Lung Collapse
The pressure within the pleural cavity (intrapleural pressure) is always negative relative to atmospheric pressure, preventing lung collapse. If this pressure equalizes with atmospheric pressure (e.g., due to a chest wound), the lung collapses (atelectasis).
Respiratory Volumes and Capacities
Respiratory volumes are measured to assess lung function. These include:
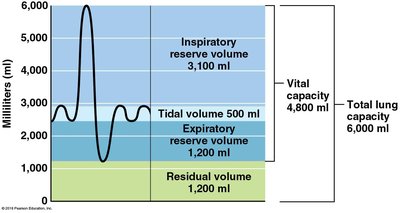
Tidal Volume (TV): Air moved during normal breathing (~500 ml).
Inspiratory Reserve Volume (IRV): Additional air inhaled after a normal inspiration (~3,100 ml).
Expiratory Reserve Volume (ERV): Additional air exhaled after a normal expiration (~1,200 ml).
Residual Volume (RV): Air remaining in lungs after maximal exhalation (~1,200 ml).
Vital Capacity (VC): Total exchangeable air (TV + IRV + ERV; ~4,800 ml in men).
Total Lung Capacity (TLC): Sum of all volumes (~6,000 ml).
Dead Space Volume: Air that does not reach alveoli (~150 ml).
Functional Volume: Air that reaches the respiratory zone (~350 ml).
Nonrespiratory Air Movements
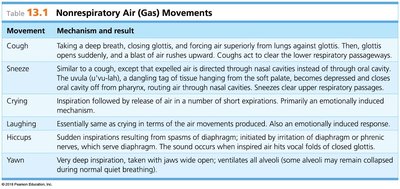
Not all air movements are involved in gas exchange. Nonrespiratory movements include coughing, sneezing, crying, laughing, hiccups, and yawning. These are often reflexive and serve to clear airways or ventilate alveoli.
Movement | Mechanism and Result |
|---|---|
Cough | Deep breath, closing glottis, forcing air out; clears lower respiratory passages. |
Sneeze | Similar to cough, but air directed through nasal cavities; clears upper passages. |
Crying | Inspiration followed by release of air in short expirations; emotionally induced. |
Laughing | Similar to crying; emotionally induced. |
Hiccups | Sudden inspirations from diaphragm spasms; sound from closing glottis. |
Yawning | Very deep inspiration; ventilates all alveoli. |
Gas Exchange and Transport
External and Internal Respiration
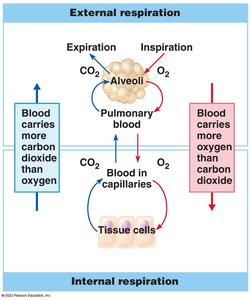
Gas exchange occurs by diffusion, moving from areas of higher to lower concentration:
External respiration: Oxygen diffuses from alveoli into pulmonary capillaries; carbon dioxide diffuses from blood into alveoli.
Internal respiration: Oxygen diffuses from blood into tissues; carbon dioxide diffuses from tissues into blood.
Transport of Gases in the Blood
Oxygen: Mostly transported bound to hemoglobin as oxyhemoglobin (HbO2); a small amount is dissolved in plasma.
Carbon dioxide: Mainly transported as bicarbonate ion (HCO3-) in plasma, which is important for buffering blood pH. Some CO2 is bound to hemoglobin (at a different site than O2), and a small amount is dissolved in plasma.
The conversion of CO2 to bicarbonate occurs in red blood cells, catalyzed by the enzyme carbonic anhydrase:
CO2 + H2O → H2CO3 → H+ + HCO3-
To release CO2 in the lungs, the reaction reverses, and CO2 diffuses into the alveoli for exhalation.
Control of Respiration
Neural Regulation
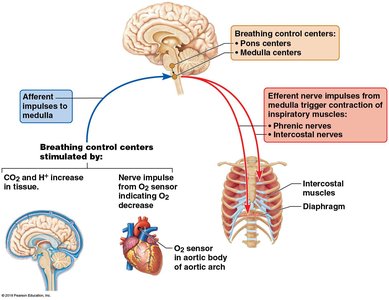
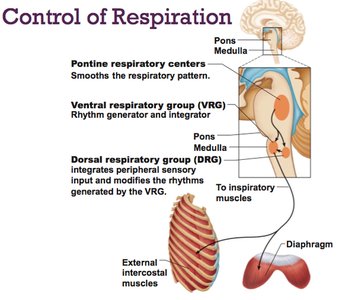
Breathing is primarily controlled by centers in the brainstem:
Medulla oblongata: Contains the ventral respiratory group (VRG) and dorsal respiratory group (DRG).
VRG: Rhythm generator for normal breathing (eupnea).
DRG: Integrates sensory input and modifies VRG rhythms.
Pons: Modifies and smooths the respiratory pattern.
Chemical and Physical Regulation
Chemoreceptors: Detect changes in CO2, O2, and pH in blood and cerebrospinal fluid. Increased CO2 (or decreased pH) stimulates increased rate and depth of breathing.
Physical factors: Exercise, body temperature, and talking can modify breathing patterns.
Voluntary control: Limited; overridden by the brainstem if blood O2 drops or CO2 rises excessively.
Emotional factors: Limbic system influences breathing during emotional responses.
Homeostatic Imbalances
Hyperventilation: Excessive breathing lowers CO2 and raises blood pH (alkalosis).
Hypoventilation: Slow, shallow breathing increases CO2 and lowers blood pH (acidosis).
Apnea: Temporary cessation of breathing, often following hyperventilation.
Cyanosis: Bluish discoloration of skin due to inadequate oxygenation.
Summary Table: Key Respiratory Volumes
Volume/Capacity | Definition | Typical Value (ml) |
|---|---|---|
Tidal Volume (TV) | Normal breath in/out | 500 |
Inspiratory Reserve Volume (IRV) | Max air inhaled after TV | 3,100 |
Expiratory Reserve Volume (ERV) | Max air exhaled after TV | 1,200 |
Residual Volume (RV) | Air remaining after max exhale | 1,200 |
Vital Capacity (VC) | TV + IRV + ERV | 4,800 (men) |
Total Lung Capacity (TLC) | Sum of all volumes | 6,000 |
Key Equations
Boyle's Law:
Vital Capacity:
CO2 Transport:
