 Back
BackThe Heart: Structure, Function, and Physiology
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
The Heart: Structure, Function, and Physiology
Introduction to the Heart
The heart is the central organ of the cardiovascular system, responsible for pumping blood throughout the body. It beats approximately 100,000 times per day, moving about 8,000 liters of blood. The heart works in conjunction with blood vessels to maintain the circulation necessary for tissue health and homeostasis.
Anatomy of the Heart
Cardiovascular Circuits
Pulmonary Circuit: Carries blood to and from the gas exchange surfaces of the lungs.
Systemic Circuit: Carries blood to and from the rest of the body.
Each circuit begins and ends at the heart, and blood travels through these circuits in sequence.

Types of Blood Vessels
Arteries: Carry blood away from the heart.
Veins: Return blood to the heart.
Capillaries: Interconnect the smallest arteries and veins, facilitating exchange of gases, nutrients, and wastes.
Chambers of the Heart
Right Atrium: Receives blood from the systemic circuit.
Right Ventricle: Pumps blood into the pulmonary circuit.
Left Atrium: Receives blood from the pulmonary circuit.
Left Ventricle: Pumps blood into the systemic circuit.
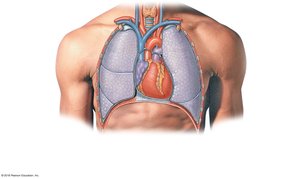
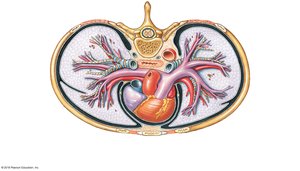
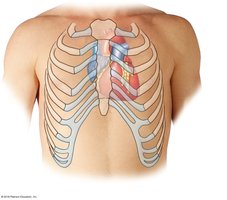
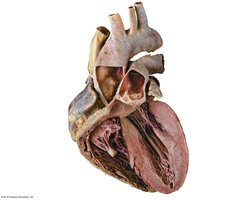
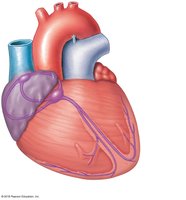
Location and Structure of the Heart
The heart is located in the mediastinum, between the two pleural cavities.
The base is superior, where great vessels connect; the apex is the pointed inferior tip.

Pericardium
Fibrous Pericardium: Outer tough connective tissue layer.
Serous Pericardium: Inner double-layered membrane (parietal and visceral layers).
Pericardial Cavity: Space between layers containing pericardial fluid to reduce friction.
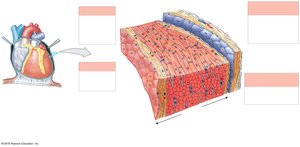
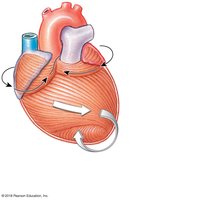
Heart Wall Layers
Epicardium: Visceral layer of serous pericardium, covers the heart surface.
Myocardium: Cardiac muscle tissue, responsible for contraction.
Endocardium: Inner lining of the heart, composed of simple squamous epithelium and areolar tissue.
Connective Tissues and Cardiac Skeleton
Support cardiac muscle fibers, blood vessels, and nerves.
Distribute contraction forces, add strength, prevent overexpansion, and provide elasticity.
Cardiac Skeleton: Four dense bands of tough elastic tissue encircle heart valves and bases of pulmonary trunk and aorta, stabilizing positions and electrically insulating atria from ventricles.
Internal Anatomy and Valves
Septa: Interatrial septum separates atria; interventricular septum separates ventricles (thicker).
Atrioventricular (AV) Valves: Tricuspid (right) and mitral (left) valves permit one-way blood flow from atria to ventricles.
Semilunar Valves: Pulmonary and aortic valves prevent backflow into ventricles.
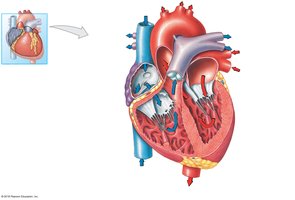
Major Blood Vessels
Superior Vena Cava: Returns blood from head, neck, upper limbs, and chest to right atrium.
Inferior Vena Cava: Returns blood from trunk, viscera, and lower limbs to right atrium.
Pulmonary Trunk: Receives blood from right ventricle, divides into left and right pulmonary arteries.
Pulmonary Veins: Return oxygenated blood from lungs to left atrium.
Aorta: Receives blood from left ventricle, distributes to systemic circuit.
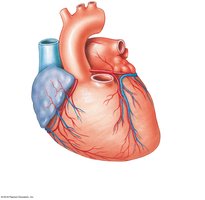
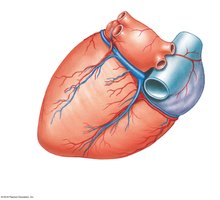
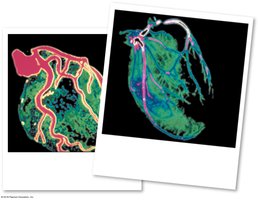
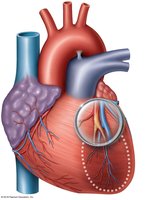
Coronary Circulation
Coronary arteries and veins supply blood to and drain blood from the myocardium. The right and left coronary arteries arise from the aortic sinuses and branch to supply the heart muscle. Cardiac veins collect deoxygenated blood and return it to the right atrium via the coronary sinus.

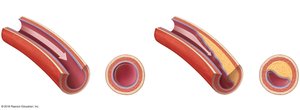
Coronary Artery Disease (CAD) and Myocardial Infarction (MI)
CAD: Partial or complete blockage of coronary circulation, usually due to atherosclerotic plaque.
Angina Pectoris: Chest pain due to temporary ischemia during increased workload.
Myocardial Infarction (Heart Attack): Blockage leads to death of cardiac muscle cells, forming a nonfunctional area (infarct).
Diagnosis includes ECG and blood studies for cardiac enzymes (troponin T, troponin I, CK-MB).
Treatments include lifestyle modification, drugs (anticoagulants, beta-blockers, vasodilators), and surgical interventions (angioplasty, stents, coronary artery bypass graft).
The Conducting System of the Heart
Cardiac Muscle Cell Types
Autorhythmic Cells: Control and coordinate heartbeat (pacemaker and conducting cells).
Contractile Cells: Produce contractions that propel blood.
Components of the Conducting System
Sinoatrial (SA) Node: Pacemaker in right atrium wall; initiates heartbeat.
Atrioventricular (AV) Node: Junction between atria and ventricles; delays impulse.
AV Bundle, Bundle Branches, Purkinje Fibers: Distribute impulse through ventricles.
Pacemaker Potential and Sinus Rhythm
Pacemaker cells have a gradual depolarization (pacemaker potential) and lack a stable resting membrane potential.
SA node sets the sinus rhythm (60–100 action potentials/min); AV node (40–60/min).
Parasympathetic stimulation slows heart rate.
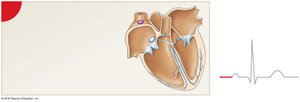
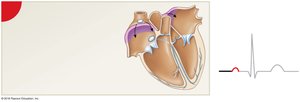
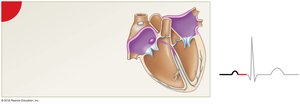
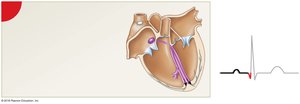
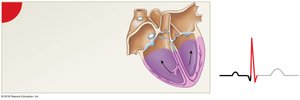
Impulse Conduction and ECG
Impulse spreads from SA node across atria to AV node (delayed 100 msec), then through AV bundle, bundle branches, Purkinje fibers, and ventricular myocardium.
Electrocardiogram (ECG): Records electrical events; key features include P wave (atrial depolarization), QRS complex (ventricular depolarization), and T wave (ventricular repolarization).
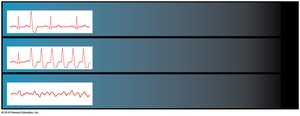
Cardiac Arrhythmias
Bradycardia: Abnormally slow heart rate.
Tachycardia: Abnormally fast heart rate.
Ectopic Pacemaker: Abnormal cells generate high rate of action potentials, disrupting normal rhythm.

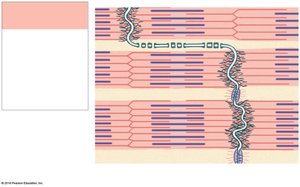
Cardiac Contractile Cells
Form bulk of atrial and ventricular walls; receive stimulus from Purkinje fibers.
Resting membrane potential: –90 mV (ventricular), –80 mV (atrial).
Intercalated discs connect cells via desmosomes and gap junctions, allowing force and action potential propagation.


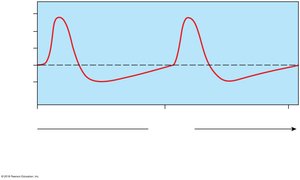
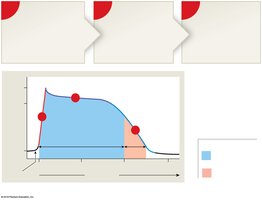
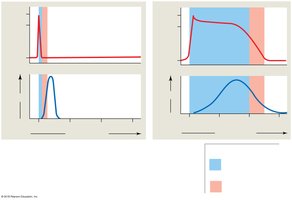
Action Potential in Cardiac Contractile Cells
Rapid Depolarization: Na+ influx through fast sodium channels.
Plateau: Ca2+ influx through slow calcium channels.
Repolarization: K+ efflux through slow potassium channels.
Refractory Period: Absolute (200 msec, no response) and relative (50 msec, strong stimulus needed); prevents tetany.
Role of Calcium Ions
Extracellular Ca2+ entry during plateau phase triggers further Ca2+ release from sarcoplasmic reticulum, essential for contraction.
Cardiac muscle is sensitive to extracellular Ca2+ levels.
Energy for Cardiac Contractions
Cardiac muscle relies on aerobic metabolism of fatty acids and glucose; oxygen is delivered by coronary circulation and stored in myoglobin.
The Cardiac Cycle
Phases of the Cardiac Cycle
Systole: Contraction phase (blood is ejected).
Diastole: Relaxation phase (chambers fill with blood).
At 75 bpm, the cardiac cycle lasts about 800 msec.
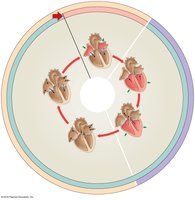
Events of the Cardiac Cycle
Atrial Systole: Atria contract, AV valves open, blood moves into ventricles.
Ventricular Systole: Ventricles contract, AV valves close (isovolumetric contraction), semilunar valves open, blood ejected (stroke volume).
Ventricular Diastole: Ventricles relax, semilunar valves close, AV valves open, passive filling occurs.
Heart Sounds
S1 ("Lubb"): AV valves close.
S2 ("Dupp"): Semilunar valves close.
S3, S4: Soft sounds from blood flow and atrial contraction.
Heart Murmur: Abnormal sounds due to valve regurgitation.
Cardiac Output
Definition and Formula
Cardiac Output (CO): Volume of blood pumped by the left ventricle per minute.
Formula:
Where is heart rate (beats/min) and is stroke volume (mL/beat).
Stroke Volume (SV)
Formula:
End-Diastolic Volume (EDV): Blood in ventricle at end of diastole.
End-Systolic Volume (ESV): Blood remaining after systole.
Ejection Fraction: Percentage of EDV ejected during contraction.
Factors Affecting Heart Rate
Autonomic Innervation: Sympathetic (increases HR) and parasympathetic (decreases HR) via cardiac plexus and medullary centers.
Hormones: Epinephrine, norepinephrine, and thyroid hormone increase HR.
Bainbridge Reflex: Increased venous return stretches right atrium, increasing HR via sympathetic stimulation.
Factors Affecting Stroke Volume
Preload: Degree of ventricular stretching during diastole (proportional to EDV).
Contractility: Force produced during contraction at a given preload (increased by sympathetic stimulation and hormones).
Afterload: Tension required to open semilunar valves and eject blood (increased afterload decreases SV).
Frank–Starling Principle
As EDV increases, stroke volume increases, up to physical limits set by myocardial connective tissues, cardiac skeleton, and pericardium.
Cardiac Reserve
Difference between resting and maximal cardiac output; indicates the heart's ability to respond to increased demands.
Summary Table: Factors Affecting Cardiac Output
Factor | Effect on Cardiac Output |
|---|---|
Heart Rate (HR) | Increased by sympathetic stimulation, hormones, increased venous return; decreased by parasympathetic stimulation |
Stroke Volume (SV) | Increased by higher EDV (preload), increased contractility, lower afterload; decreased by lower EDV, reduced contractility, higher afterload |
Autonomic Nervous System | Sympathetic increases HR and contractility; parasympathetic decreases HR |
Hormones | Epinephrine, norepinephrine, thyroid hormone increase HR and contractility |
Additional info: This guide covers the essential anatomy and physiology of the heart, including its structure, function, conduction system, cardiac cycle, and regulation of cardiac output. It is suitable for exam preparation in a college-level Anatomy & Physiology course.
