 Back
BackThe Peripheral Nervous System: Structure, Function, and Clinical Correlates
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
The Peripheral Nervous System (PNS)
Overview of the Peripheral Nervous System
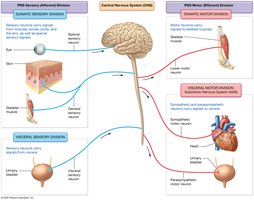
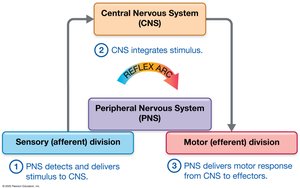
The Peripheral Nervous System (PNS) serves as the communication link between the Central Nervous System (CNS) and the rest of the body, including the external environment. It detects sensory stimuli and delivers them to the CNS as sensory input, which is then processed and relayed back through the PNS to effectors (muscle cells and glands) for motor output. Both spinal nerves and cranial nerves are part of the PNS, even though they attach directly to the spinal cord and brain.
Divisions of the PNS
Sensory (Afferent) Division
Somatic Sensory Division: Carries signals from muscles, bones, joints, skin, and special sensory signals to the CNS.
Visceral Sensory Division: Carries signals from organs of the thoracic and abdominopelvic cavities to the CNS.
Motor (Efferent) Division
Somatic Motor Division: Carries signals to skeletal muscles.
Visceral Motor Division (Autonomic Nervous System, ANS): Carries signals to cardiac and smooth muscles and glands.
Sympathetic Nervous System: "Fight or Flight" system.
Parasympathetic Nervous System: "Rest and Digest" system.
Peripheral Nerves and Associated Ganglia
Structure of Peripheral Nerves
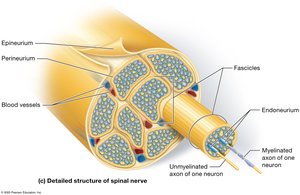
Peripheral nerves are bundles of axons from many neurons, bound together by connective tissue sheaths. They innervate most body structures and are classified as:
Mixed nerves: Contain both sensory and motor axons.
Sensory nerves: Contain only sensory axons.
Motor nerves: Contain mostly motor axons, with some sensory axons for monitoring muscle stretch and tension.
Cranial nerves attach to the brain and innervate the head and neck, while spinal nerves branch from the spinal cord and innervate structures below the neck.
Connective Tissue Sheaths of Nerves
Epineurium: Surrounds the entire nerve.
Perineurium: Surrounds each fascicle (bundle of axons).
Endoneurium: Surrounds individual axons.

Cranial Nerves
Overview and Classification
There are 12 pairs of cranial nerves, each with specific sensory, motor, or mixed functions. They are often remembered by mnemonics for their order and function. Cranial nerves can be classified as:
Sensory only: Olfactory, Optic, Vestibulocochlear
Motor only: Oculomotor, Trochlear, Abducens, Accessory, Hypoglossal
Mixed: Trigeminal, Facial, Glossopharyngeal, Vagus

Selected Cranial Nerve Disorders
Trigeminal Neuralgia: Chronic pain syndrome affecting the trigeminal nerve, causing brief, intense, unilateral facial pain. Triggers include chewing or light touch. Treatment may involve anticonvulsant drugs.
Bell’s Palsy: Rapid-onset weakness or paralysis of facial muscles due to impairment of the facial nerve, often affecting one side. Symptoms include difficulty closing the eye and making facial expressions. Most recover within weeks, sometimes with medication or therapy.

Spinal Nerves and Plexuses
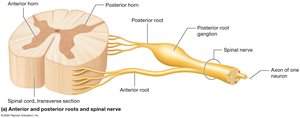
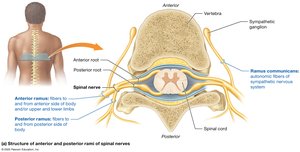
Structure and Branches of Spinal Nerves
There are 31 pairs of spinal nerves classified by region: cervical (8), thoracic (12), lumbar (5), sacral (5), and coccygeal (1). Each spinal nerve splits into:
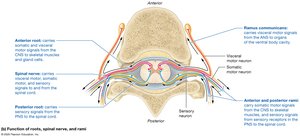
Posterior ramus: Serves the posterior body.
Anterior ramus: Serves the anterior body and limbs; forms nerve plexuses in cervical, lumbar, and sacral regions.
Ramus communicans: Contains autonomic (visceral motor) axons of the sympathetic nervous system.
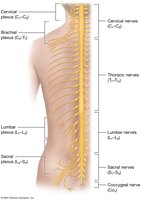
Cervical Plexus
The cervical plexus is formed by the anterior rami of C1–C4 (with some C5 and hypoglossal nerve contributions). It supplies sensory and motor branches to the neck, head, chest, and shoulders. The phrenic nerve (C3–C5) is a major motor branch, innervating the diaphragm.

Brachial Plexus
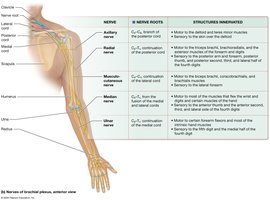
The brachial plexus arises from the anterior rami of C5–T1 and innervates the upper limb. It is organized into trunks, divisions, cords, and branches. The five major nerves are:
Axillary nerve: Deltoid and teres minor muscles; skin over deltoid.
Radial nerve: Posterior arm/forearm, triceps brachii, extensors.
Musculocutaneous nerve: Biceps brachii, brachialis; lateral forearm skin.
Median nerve: Most wrist/digit flexors; anterior thumb and lateral digits.
Ulnar nerve: Intrinsic hand muscles; medial hand and digits.

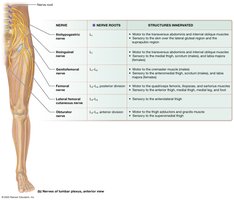
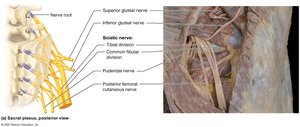
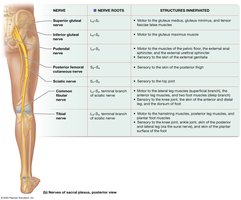
Lumbar and Sacral Plexuses
The lumbar plexus (L1–L4) supplies the pelvis and lower extremity. Major nerves include the obturator nerve (thigh adductors) and femoral nerve (anterior thigh muscles). The sacral plexus (L4–S4) supplies the pelvis, gluteal region, and lower limb. The sciatic nerve is the largest nerve, splitting into the tibial and common fibular nerves.

Sensory Receptors and Sensation
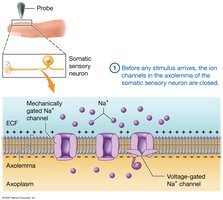
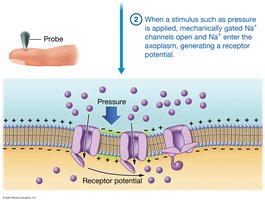
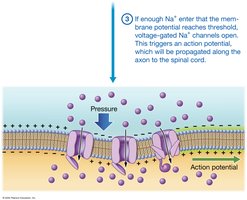
Sensory Transduction and Receptor Types
Sensory transduction is the conversion of a stimulus into an electrical signal at a sensory receptor. Sensory receptors can be:
Encapsulated nerve endings: Surrounded by supporting cells.
Free nerve endings: Lacking supportive cells.
Receptors are classified by location (exteroceptors, interoceptors) and stimulus type (mechanoreceptors, thermoreceptors, chemoreceptors, photoreceptors, nociceptors).
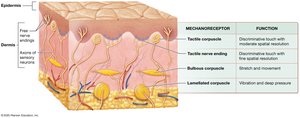
Mechanoreceptors in the Skin
Tactile (Merkel) nerve endings: Discriminative touch, high spatial resolution.
Tactile (Meissner) corpuscles: Discriminative touch, less fine than Merkel endings.
Bulbous corpuscles (Ruffini endings): Stretch and movement.
Lamellated corpuscles (Pacinian): Vibration and deep pressure.
Hair follicle receptors: Hair movement.
Proprioceptors: Detect body position and movement.
Somatic Sensory Neurons and Sensory Fields
Structure and Function of Sensory Neurons
First-order somatic sensory neurons are pseudounipolar, with a cell body in the posterior root ganglion, a peripheral process with sensory receptors, and a central process entering the CNS. The speed of action potential conduction depends on axon diameter and myelination.

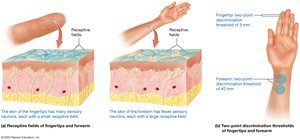
Receptive Fields and Dermatomes
Receptive field: Area served by a neuron; small fields allow finer sensation (e.g., fingertips).
Two-point discrimination: Measures receptive field size.
Dermatomes: Skin regions supplied by specific spinal nerves; used clinically to assess sensory pathway integrity.
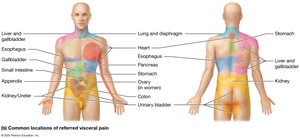
Referred pain: Pain from an organ perceived as cutaneous pain due to shared spinal nerve pathways.

Motor Output and Reflexes
Motor Pathways
Skeletal muscle contraction is initiated by somatic motor neurons. The CNS initiates movement via upper motor neurons, which relay signals to lower motor neurons. Lower motor neurons release acetylcholine to stimulate muscle contraction.




Reflex Arcs
A reflex is a programmed, automatic response to sensory input, often protective. Reflexes can be:
Monosynaptic: Single synapse (e.g., stretch reflex).
Polysynaptic: Multiple synapses (e.g., withdrawal reflex).
Somatic: Involving skeletal muscles.
Visceral: Involving internal organs (autonomic).
Types of Somatic Reflexes
Simple stretch reflex: Maintains muscle length (e.g., patellar reflex).
Flexion (withdrawal) and crossed-extension reflexes: Withdraw from pain and maintain balance.
Golgi tendon reflex: Prevents muscle/tendon damage by causing relaxation under excessive tension.
Cranial nerve reflexes: Involve cranial nerves (e.g., gag reflex, corneal blink reflex).
Clinical Correlates: Peripheral Neuropathies and ALS
Peripheral Neuropathies
Peripheral neuropathies are disorders affecting sensory and motor neurons of the PNS. Symptoms depend on the nerves involved and may include paralysis, weakness, or sensory loss. Upper motor neuron disorders affect CNS pathways and can result in spasticity and abnormal reflexes (e.g., Babinski sign).
Amyotrophic Lateral Sclerosis (ALS)
ALS is a neurodegenerative disease affecting both upper and lower motor neurons, leading to progressive muscle weakness and, in many cases, cognitive changes. Death typically occurs within five years of onset.
