 Back
BackThe Respiratory System: Structure, Function, and Physiology
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
The Respiratory System
Overview and Functions
The respiratory system is essential for gas exchange, supplying oxygen to the body and removing carbon dioxide. This process involves several coordinated steps and anatomical structures, integrating principles from chemistry, physics, and biology.
Pulmonary ventilation: Movement of air into and out of the lungs.
External respiration: Gas exchange between the air in the alveoli and the blood.
Transport of gases: Movement of oxygen and carbon dioxide in the blood.
Internal respiration: Gas exchange between blood and tissues.
Anatomy of the Respiratory System
Major Structures and Pathways
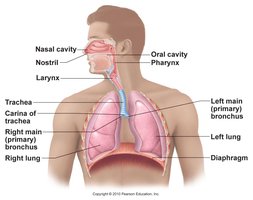
Air enters through the nasal or oral cavity, passes through the pharynx, larynx, trachea, and then into the bronchial tree, eventually reaching the alveoli where gas exchange occurs.
Pharynx: Passageway for both air and food.
Larynx: Air passageway containing vocal cords; separates air and food.
Trachea: Flexible tube with hyaline cartilage rings; humidifies, warms, and filters air.
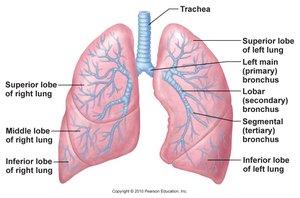
Bronchi: Right and left primary bronchi branch into secondary and tertiary bronchi, then into bronchioles and alveolar sacs.
The Conducting and Respiratory Zones
The respiratory tract is divided into the conducting zone (air movement, no gas exchange) and the respiratory zone (site of gas exchange).
Conducting zone: Nasal cavity to terminal bronchioles; warms, filters, and humidifies air.
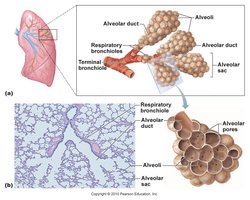
Respiratory zone: Respiratory bronchioles, alveolar ducts, and alveolar sacs; site of gas exchange.

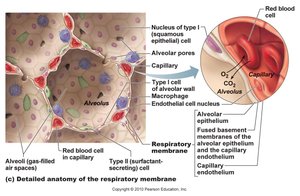
Alveoli and the Respiratory Membrane
Alveoli are tiny sacs providing a large surface area for gas exchange. Their walls are composed of:
Type I alveolar cells: Simple squamous epithelial cells forming the structure of the alveolar wall.
Type II alveolar cells: Secrete surfactant to reduce surface tension.
Alveolar macrophages: Phagocytize debris and pathogens.
The respiratory membrane is extremely thin, allowing efficient diffusion of gases between alveoli and capillaries.
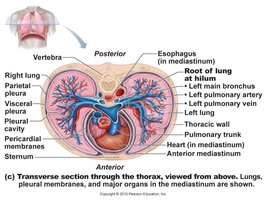
Pleural Membranes
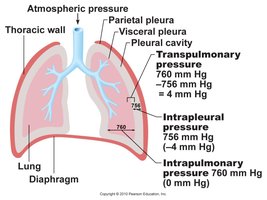
The lungs are surrounded by serous membranes called pleurae:
Visceral pleura: Covers the lungs.
Parietal pleura: Lines the thoracic cavity.
Pleural cavity: Contains lubricating serous fluid, reducing friction and creating a vacuum to keep lungs expanded.
Physical Properties of the Lungs
Compliance and Elasticity
Lung compliance refers to the ability of the lungs to expand in response to pressure changes. High compliance means the lungs expand easily; low compliance means they are stiff.
Elastic fibers: Provide recoil, causing lungs to collapse when not held open by pleural vacuum.
Surface tension: Water lining alveoli creates inward force; surfactant reduces this tension.
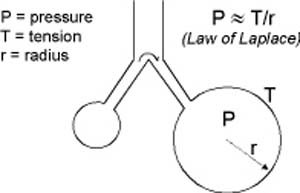
Law of LaPlace
The Law of LaPlace describes the relationship between pressure, surface tension, and radius in alveoli:
Equation:
Smaller alveoli would collapse into larger ones without surfactant.
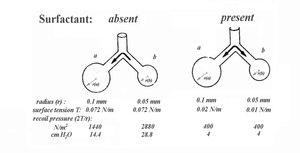
Role of Surfactant
Surfactant, produced by Type II alveolar cells, reduces surface tension, stabilizing alveoli and preventing collapse, especially in smaller alveoli.
Lung Diseases Affecting Compliance
Fibrosis: Scar tissue reduces compliance, making lungs harder to inflate.
Emphysema: Destruction of alveolar walls reduces surface area and elastic recoil, increasing compliance but impairing exhalation.
Mechanics of Breathing
Boyle’s Law and Air Movement
Boyle’s Law states that pressure and volume are inversely related: . Changes in thoracic volume drive air movement.
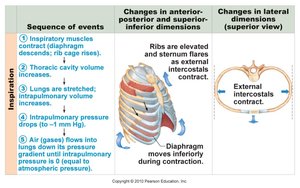
Inhalation (Inspiration)
Inhalation is an active process involving contraction of the diaphragm and external intercostal muscles, increasing thoracic volume and decreasing intrapulmonary pressure, drawing air in.
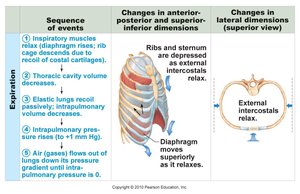
Exhalation (Expiration)
Exhalation is usually passive, relying on elastic recoil to decrease thoracic volume and increase pressure, pushing air out. Forced expiration uses internal intercostals and abdominal muscles.
Airway Resistance
Airflow is determined by the pressure gradient and airway resistance:
Equation:
Resistance is inversely proportional to the fourth power of airway radius:
Bronchoconstriction (e.g., asthma) greatly increases resistance and reduces airflow.
Respiratory Volumes and Capacities
Spirometry and Lung Volumes
Spirometry measures lung volumes and capacities, important for assessing respiratory health.
Tidal Volume (TV): Normal breath in and out (~500 mL).
Inspiratory Reserve Volume (IRV): Extra air inhaled after normal inspiration.
Expiratory Reserve Volume (ERV): Extra air exhaled after normal expiration.
Residual Volume (RV): Air remaining after maximal exhalation.
Total Lung Capacity (TLC): TV + IRV + ERV + RV.
Vital Capacity (VC): TV + IRV + ERV.
Gas Laws and Gas Exchange
Dalton’s Law of Partial Pressures
Dalton’s Law states that the total pressure of a gas mixture equals the sum of the partial pressures of each component gas. The partial pressure of a gas is proportional to its concentration in the mixture.
Equation:
Example: Atmospheric pressure is 760 mmHg; if O2 is 21%, mmHg.
Henry’s Law
Henry’s Law relates the solubility of a gas in a liquid to its partial pressure and temperature:
Equation:
Higher partial pressure increases solubility; higher temperature decreases solubility.
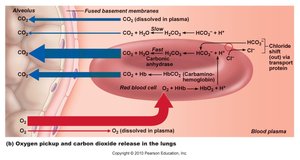
Gas Exchange in Alveoli and Tissues
Gas exchange is driven by differences in partial pressures:
O2 diffuses from alveoli (PO2 104 mmHg) to blood (PO2 40 mmHg).
CO2 diffuses from blood (PCO2 45 mmHg) to alveoli (PCO2 40 mmHg).
In tissues, O2 leaves blood for tissues, CO2 enters blood from tissues.

Transport of Respiratory Gases
Oxygen Transport
Oxygen is transported in two forms:
1.5% dissolved in plasma.
98.5% bound to hemoglobin (Hb) as oxyhemoglobin (HbO2).
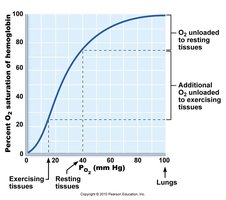
The binding and release of O2 from Hb is reversible and depends on PO2:
High PO2 (lungs): Hb binds O2 tightly (high affinity).
Low PO2 (tissues): Hb releases O2 (low affinity).
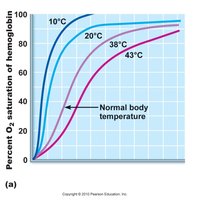
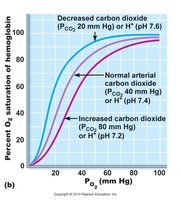
Temperature and pH also affect Hb affinity for O2 (Bohr effect):
Increased temperature or decreased pH (more acidic) lowers affinity, promoting O2 release.
Types of Hypoxia
Anemic hypoxia: Low Hb or RBC count.
Ischemic hypoxia: Inadequate blood flow.
Histotoxic hypoxia: Cells unable to use O2 (e.g., cyanide poisoning).
Hypoxemic hypoxia: Low arterial PO2 (e.g., high altitude).
Carbon monoxide poisoning: CO binds Hb more tightly than O2.
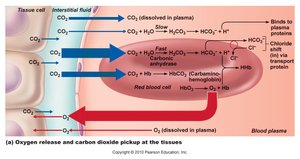
Carbon Dioxide Transport
CO2 is transported in three forms:
10% dissolved in plasma.
20% bound to Hb as carbaminohemoglobin.
70% as bicarbonate ion (HCO3-) via the carbonic acid-bicarbonate buffer system:

Breathing and Blood pH
CO2 levels influence blood pH. Increased CO2 leads to increased H+ (lower pH, acidosis); decreased CO2 leads to decreased H+ (higher pH, alkalosis).
Control of Breathing
Neural Control Centers
Breathing is regulated by centers in the medulla and pons:
Ventral Respiratory Group (VRG): Controls basic rhythm of breathing.
Dorsal Respiratory Group (DRG): Integrates sensory input and modifies VRG output.
Pontine Respiratory Group (PRG): Modifies and smooths respiratory rhythm.
Chemical Regulation
CO2 is the primary chemical regulator of breathing. Central chemoreceptors in the medulla respond to changes in pH of cerebrospinal fluid, which reflects CO2 levels. Peripheral chemoreceptors in the aortic and carotid bodies respond to low O2 and low pH.
Increased CO2 (hypercapnia) stimulates increased ventilation.
Decreased CO2 (hypocapnia) reduces ventilation.
Low O2 (< 60 mmHg) also stimulates increased ventilation.
Role in Acid-Base Balance
The respiratory system helps maintain blood pH (7.35–7.45) by regulating CO2 exhalation. Hypoventilation causes acidosis; hyperventilation causes alkalosis.
Additional info: These notes integrate anatomical, physiological, and biochemical principles relevant to the respiratory system, suitable for college-level Anatomy & Physiology students. All images included are directly relevant to the adjacent content and reinforce key concepts.
