 Back
BackThe Urinary System: Structure and Function of the Kidneys
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
The Urinary System
Overview and Major Functions
The urinary system is essential for maintaining the body's internal environment by regulating water, solute concentrations, and removing metabolic wastes. It consists of the kidneys, ureters, urinary bladder, and urethra.
Regulation of water and solute balance: Kidneys control total water volume and solute concentration in the body.
Ion regulation: Maintains ion concentrations in extracellular fluid (ECF).
Acid-base balance: Ensures long-term acid-base equilibrium.
Excretion: Removes metabolic wastes, toxins, and drugs.
Hormone production: Produces erythropoietin (stimulates RBC production) and renin (regulates blood pressure).
Other functions: Activates vitamin D and can perform gluconeogenesis if needed.
Gross Anatomy of the Kidneys
Location and External Anatomy
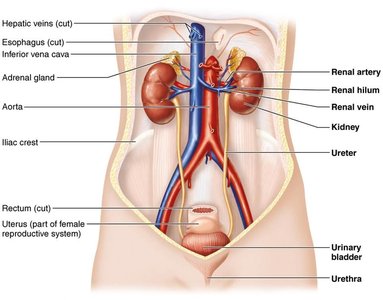
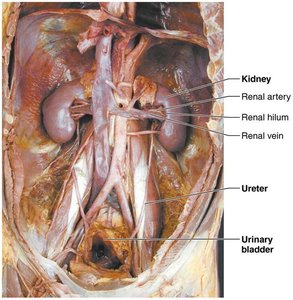
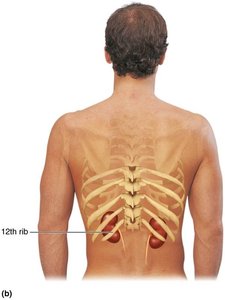
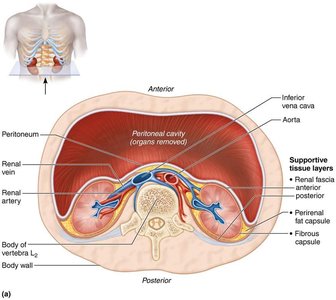
The kidneys are retroperitoneal organs located in the superior lumbar region, between vertebrae T12 and L5. The right kidney is slightly lower due to the liver. Each kidney is capped by an adrenal gland and has a convex lateral surface and a concave medial surface with a vertical renal hilum, where vessels, nerves, and the ureter enter or exit.
Supportive tissue layers:
Renal fascia: Anchoring outer layer of dense fibrous connective tissue.
Perirenal fat capsule: Fatty cushion for protection.
Fibrous capsule: Transparent capsule preventing infection spread.
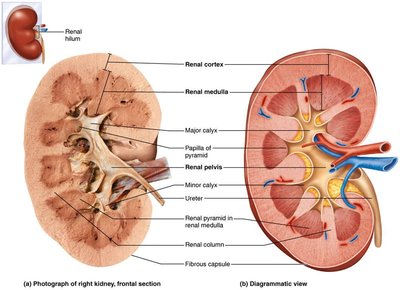
Internal Gross Anatomy
Internally, the kidney has three main regions:
Renal cortex: The outer, granular-appearing region.
Renal medulla: Contains cone-shaped renal pyramids separated by renal columns. Each pyramid and its surrounding cortex form a lobe (about 8 per kidney).
Renal pelvis: Funnel-shaped tube continuous with the ureter. Minor calyces collect urine from pyramids, major calyces collect from minor calyces, and urine flows into the renal pelvis and then the ureter.
Clinical Note: Homeostatic Imbalances
Trauma: Lower parts of kidneys are susceptible to blunt trauma (e.g., falls, car accidents). The renal artery is vulnerable to injury, which can cause hematuria (blood in urine).
Infections: Pyelitis (infection of renal pelvis/calyces) and pyelonephritis (infection/inflammation of the entire kidney) can cause swelling, abscesses, and pus formation. Usually treated with antibiotics.
Blood and Nerve Supply of the Kidneys
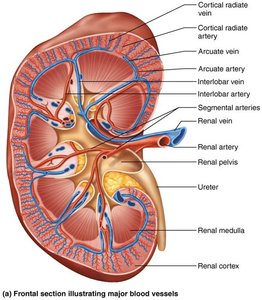
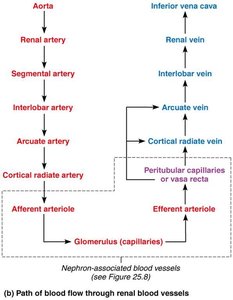
Renal Circulation
The kidneys receive about 25% of cardiac output (1200 ml/min). Blood flows through a series of arteries and veins, with the renal artery entering and the renal vein exiting at the hilum.
Arterial flow: Renal → Segmental → Interlobar → Arcuate → Cortical radiate (interlobular) arteries → Afferent arteriole → Glomerulus → Efferent arteriole
Venous flow: Cortical radiate → Arcuate → Interlobar → Renal veins (no segmental veins)
Nerve Supply
Sympathetic fibers from the renal plexus innervate the kidneys, regulating blood flow and influencing urine formation.
Nephrons: The Functional Units of the Kidney
Structure of Nephrons
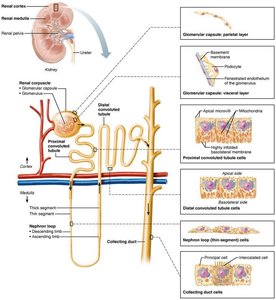
Each kidney contains over 1 million nephrons, which are responsible for urine formation. Each nephron consists of two main parts:
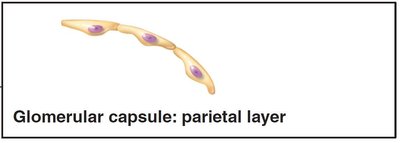
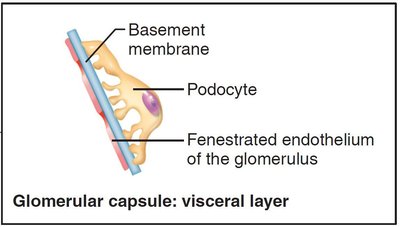
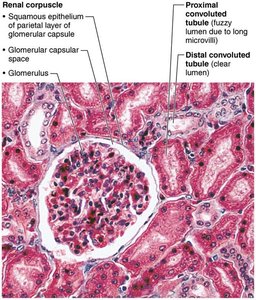
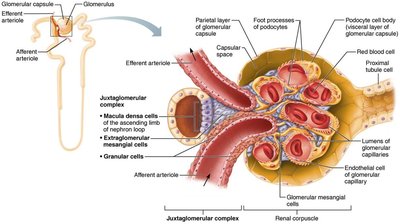
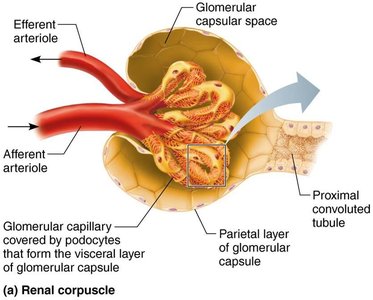
Renal corpuscle: Includes the glomerulus (a tuft of fenestrated capillaries) and the glomerular (Bowman's) capsule, which has parietal and visceral layers (the latter formed by podocytes).
Renal tubule: Composed of the proximal convoluted tubule (PCT), nephron loop (loop of Henle), and distal convoluted tubule (DCT). The DCT drains into a collecting duct.
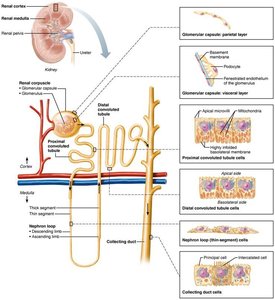
Renal Tubule and Collecting Duct
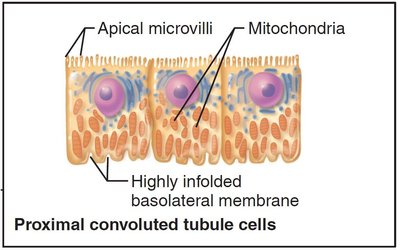
Proximal convoluted tubule (PCT): Lined with cuboidal cells with dense microvilli for reabsorption and secretion; confined to the cortex.
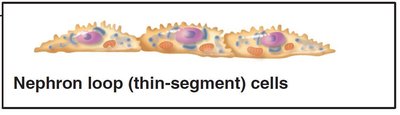
Nephron loop: U-shaped, with descending (thin, simple squamous) and ascending (thick, cuboidal/columnar) limbs.
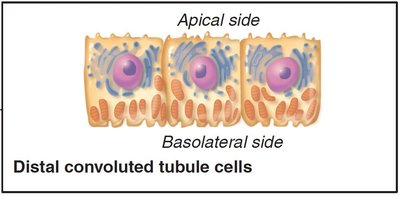
Distal convoluted tubule (DCT): Cuboidal cells with few microvilli; mainly involved in secretion; confined to the cortex.
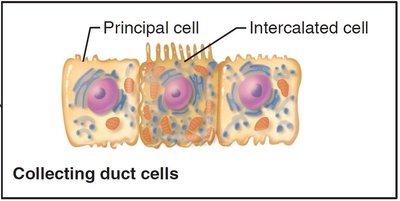
Collecting ducts: Receive filtrate from multiple nephrons, run through medullary pyramids, and fuse to deliver urine into minor calyces. Principal cells (water/Na+ balance) and intercalated cells (acid-base balance) are present.
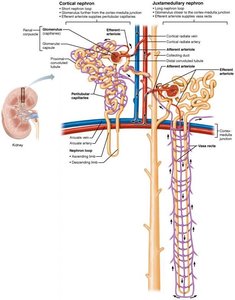
Classes of Nephrons
Cortical nephrons: 85% of nephrons; almost entirely in the cortex.
Juxtamedullary nephrons: Long nephron loops deeply invade the medulla; important for producing concentrated urine.
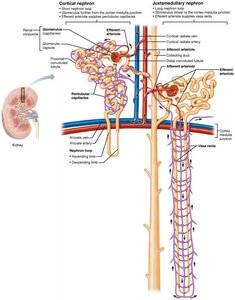
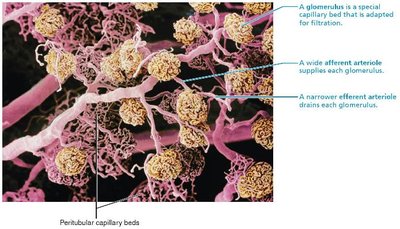
Nephron Capillary Beds
Glomerulus: Specialized for filtration; fed and drained by arterioles (afferent and efferent).
Peritubular capillaries: Low-pressure, porous capillaries for absorption; arise from efferent arterioles and surround renal tubules in the cortex.
Vasa recta: Long, thin-walled vessels parallel to nephron loops of juxtamedullary nephrons; crucial for forming concentrated urine.
Juxtaglomerular Complex (JGC)
The JGC is a specialized structure important for regulating filtrate formation and blood pressure. It involves the distal ascending limb of the nephron loop and the afferent arteriole.
Macula densa: Chemoreceptors sensing NaCl content in filtrate.
Granular (JG) cells: Mechanoreceptors sensing blood pressure; secrete renin.
Extraglomerular mesangial cells: May relay signals between macula densa and granular cells.
Physiology of the Kidney
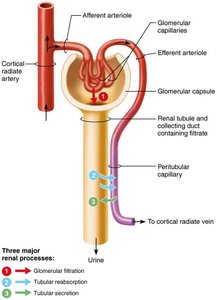
Urine Formation and Renal Processes
The kidneys process about 180 L of fluid daily, forming only 1.5 L of urine. They filter the entire plasma volume 60 times per day and consume 20–25% of resting oxygen. Urine is produced from filtrate, which is blood plasma minus proteins.
Three major processes:
Glomerular filtration: Passive process producing cell- and protein-free filtrate.
Tubular reabsorption: Selectively returns 99% of substances from filtrate to blood.
Tubular secretion: Selectively moves substances from blood to filtrate.
Glomerular Filtration
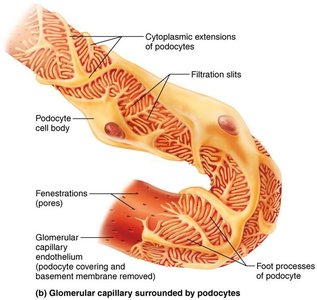
Filtration is driven by hydrostatic pressure and occurs across a filtration membrane with three layers:
Fenestrated endothelium of glomerular capillaries
Basement membrane
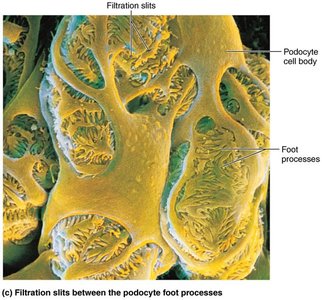
Foot processes of podocytes with filtration slits
Filtration Pressures and Glomerular Filtration Rate (GFR)
Outward pressure: Hydrostatic pressure in glomerular capillaries (HPgc, ~55 mm Hg) pushes water and solutes out of blood.
Inward pressures: Hydrostatic pressure in capsular space (HPcs, 15 mm Hg) and colloid osmotic pressure in capillaries (OPgc, 30 mm Hg) oppose filtration.
Net filtration pressure (NFP): mm Hg
GFR: Volume of filtrate formed per minute by both kidneys (normal = 120–125 ml/min). GFR is proportional to NFP, surface area, and membrane permeability.
Regulation of Glomerular Filtration
Intrinsic controls (renal autoregulation): Maintains constant GFR when mean arterial pressure is 80–180 mm Hg. Includes myogenic mechanism (smooth muscle response to stretch) and tubuloglomerular feedback (macula densa senses NaCl).
Extrinsic controls: Neural (sympathetic) and hormonal (renin-angiotensin-aldosterone) mechanisms regulate GFR to maintain systemic blood pressure.
Other factors: Paracrine chemicals (adenosine, prostaglandin E2) and local angiotensin II production can modulate GFR.
Clinical Note: Homeostatic Imbalances
Anuria: Abnormally low urine output (<50 ml/day), may indicate low glomerular blood pressure or nephron dysfunction (e.g., acute nephritis, transfusion reactions, crush injuries).
