 Back
BackThe Urinary System: Structure, Function, and Physiology
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
The Urinary System
Overview of Urinary System Structures
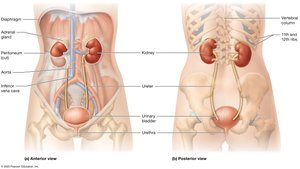
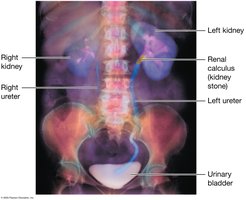
The urinary system is essential for filtering blood, removing waste, and maintaining homeostasis. It consists of paired kidneys and the urinary tract, which includes the ureters, urinary bladder, and urethra.
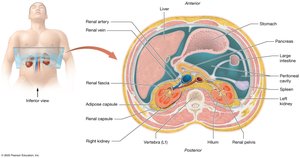
Kidneys: Retroperitoneal organs located against the posterior abdominal wall. The left kidney extends from T12 to L3, while the right sits lower due to the liver. Both are partially protected by the 11th and 12th ribs and are capped by adrenal glands.
Urinary Tract: Urine leaves the kidneys via ureters, is stored in the urinary bladder, and expelled through the urethra.
Overview of Kidney Function
The kidneys perform several vital functions to maintain the body's internal environment:
Removal of metabolic wastes: Filtering blood to eliminate waste products.
Fluid and electrolyte balance: Regulating osmolarity by conserving or eliminating water and electrolytes (e.g., sodium, potassium, calcium).
Acid-base balance: Maintaining blood pH by managing hydrogen and bicarbonate ions.
Blood pressure regulation: Influencing systemic blood pressure via blood volume control and enzyme secretion.
Regulation of erythropoiesis: Releasing erythropoietin to stimulate red blood cell production.
Other metabolic functions: Detoxification, vitamin D activation, and gluconeogenesis.
Kidney Anatomy
External Anatomy of the Kidneys
Each kidney is protected and anchored by three layers of connective tissue:
Renal Fascia: Dense irregular connective tissue anchoring the kidney.
Adipose Capsule: Middle layer of fat for shock absorption; loss can cause nephroptosis (kidney droop).
Renal Capsule: Thin, dense irregular connective tissue protecting from infection and trauma.
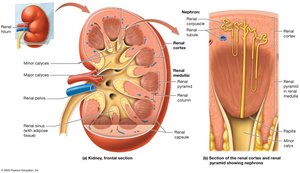
Hilum: Medial opening for vessels, nerves, and ureter.
Renal Sinus: Central cavity with urine-draining structures and adipose tissue.
Internal Anatomy of the Kidneys
The kidney is divided into three main regions:
Renal Cortex: Outer region, rich in blood vessels, contains renal columns.
Renal Medulla: Contains renal pyramids separated by columns; fewer blood vessels than cortex.
Renal Pelvis: Inner collecting chamber for urine.
Nephrons: Over one million per kidney; functional units that filter blood and produce urine.
Urine Flow: Papilla → Minor Calyx → Major Calyx → Renal Pelvis.
Blood Supply of the Kidneys
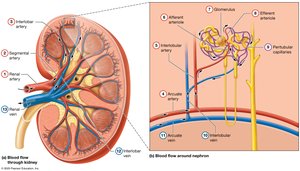
The kidneys receive about 25% of cardiac output. Blood flows through a complex network of arteries and capillaries:
Arterial Pathway: Renal artery → Segmental artery → Interlobar artery → Arcuate artery → Interlobular (cortical radiate) artery → Afferent arteriole → Glomerulus → Efferent arteriole → Peritubular capillaries.
Venous Pathway: Interlobular vein → Arcuate vein → Interlobar vein → Renal vein.
Microanatomy: The Nephron and Collecting System
Nephron Structure
Nephrons filter blood and modify filtrate through several segments:
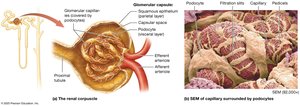
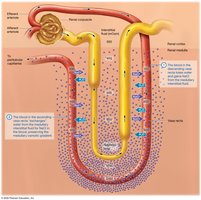
Renal Corpuscle: Includes the glomerulus (leaky capillaries with fenestrations) and Bowman's capsule (parietal and visceral layers with podocytes forming filtration slits).
Renal Tubule: Filtrate flows from the corpuscle into the tubule, which includes:
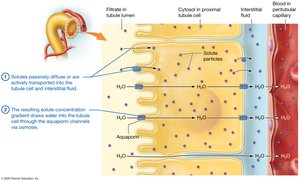
Proximal Tubule: Simple cuboidal cells with microvilli (brush border) for reabsorption.
Nephron Loop (Loop of Henle): Descending limb (water permeable), ascending limb (solute transport).
Distal Tubule: Simple cuboidal cells, fewer microvilli.


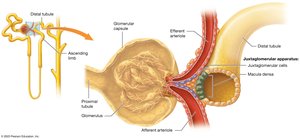
Juxtaglomerular Apparatus (JGA)
The JGA regulates blood pressure and glomerular filtration rate. It includes macula densa cells (distal tubule) and juxtaglomerular (JG) cells (afferent/efferent arterioles).
The Collecting System
Distal tubules drain into cortical collecting ducts, which merge into medullary collecting ducts and then papillary ducts. At the end of the papillary ducts, filtrate is now urine.

Types of Nephrons
Cortical Nephrons: 80% of nephrons, mostly in cortex, short loops.
Juxtamedullary Nephrons: Corpuscle near cortex-medulla boundary, long loops, surrounded by vasa recta.

Renal Physiology
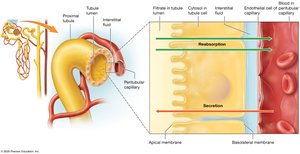
Three Basic Processes
Glomerular Filtration: Blood pressure forces plasma (minus cells/proteins) into the capsular space, forming filtrate.
Tubular Reabsorption: Water, glucose, amino acids, and electrolytes are reclaimed from filtrate back to blood, mainly in the proximal tubule and nephron loop.
Tubular Secretion: Additional substances are secreted from blood into filtrate for excretion, maintaining homeostasis and removing toxins.

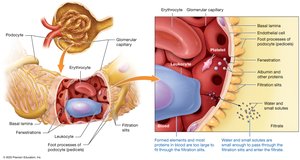
The Filtration Membrane
Fenestrated Endothelial Cells: Allow passage of most solutes but not blood cells/platelets.
Basal Lamina: Meshwork that blocks large/negatively charged proteins.
Podocytes: Form filtration slits; only small molecules (<6–7 nm) pass into filtrate.
Glomerular Filtration Rate (GFR)
GFR is the rate at which filtrate is formed (about 125 mL/min). It depends on three pressures:
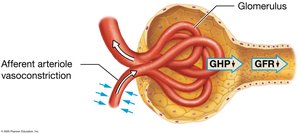
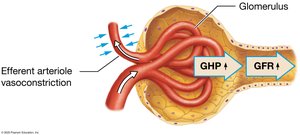
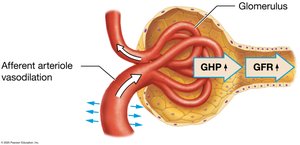
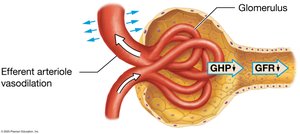
Glomerular Hydrostatic Pressure (GHP): Favors filtration (about 50 mm Hg).
Glomerular Colloid Osmotic Pressure (GCOP): Opposes filtration (about 30 mm Hg).
Capsular Hydrostatic Pressure (CHP): Opposes filtration (about 10 mm Hg).
Net Filtration Pressure (NFP):

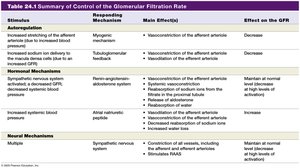
Regulation of GFR
Autoregulation: Myogenic mechanism and tubuloglomerular feedback keep GFR constant over a range of blood pressures.
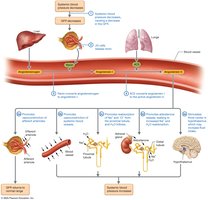
Hormonal Regulation: Renin-angiotensin-aldosterone system (RAAS) increases GFR and blood pressure; atrial natriuretic peptide (ANP) increases GFR by dilating afferent and constricting efferent arterioles.
Neural Regulation: Sympathetic stimulation can decrease GFR during stress or blood loss.
Tubular Reabsorption and Secretion
Principles of Tubular Reabsorption and Secretion
Paracellular Route: Substances pass between tubule cells (e.g., small ions, water).
Transcellular Route: Substances move through tubule cells (e.g., glucose, amino acids).
Carrier-Mediated Transport: Includes facilitated diffusion, primary and secondary active transport, antiporters, and symporters. Carrier proteins have a transport maximum.
Reabsorption and Secretion in the Proximal Tubule
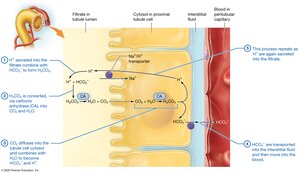
Main Roles: Reabsorption of most electrolytes, nutrients, bicarbonate, and water; secretion of hydrogen ions, nitrogenous wastes, and drugs.
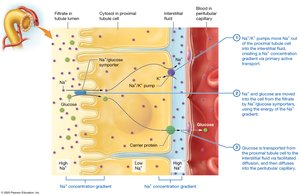
Sodium Reabsorption: Via leak channels, symporters, and antiporters.
Glucose Reabsorption: Secondary active transport with sodium, then facilitated diffusion into blood.
Bicarbonate Reabsorption: Involves the carbonic acid-bicarbonate buffer system:

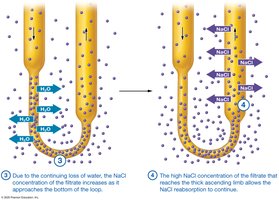
Reabsorption in the Nephron Loop
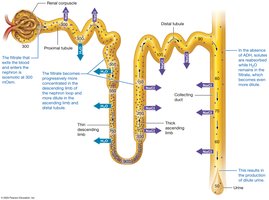
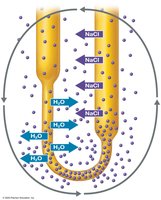
Descending Limb: Permeable to water, not solutes; filtrate becomes more concentrated.
Ascending Limb: Impermeable to water, actively transports NaCl out; filtrate becomes less concentrated.
Reabsorption and Secretion in the Distal Tubule and Collecting System
Hormone Regulation: Aldosterone increases Na+ reabsorption and K+ secretion; ADH increases water reabsorption; ANP decreases Na+ and water reabsorption.
Medullary Collecting System: Water reabsorption depends on ADH; permeable to urea; continues to reabsorb ions and secrete H+.
Osmolarity and Urine Concentration
Osmolarity of the Filtrate
Filtrate is isosmotic with plasma in the proximal tubule (~300 mOsm).
Descending limb: filtrate becomes concentrated (up to 1200 mOsm).
Ascending limb: filtrate becomes dilute (<300 mOsm).
Distal tubule and collecting system: final concentration depends on ADH and body needs.
Production of Dilute and Concentrated Urine
Dilute Urine: Low ADH, collecting ducts impermeable to water, urine as dilute as 50 mOsm.
Concentrated Urine: High ADH, water reabsorbed, urine up to 1200 mOsm.
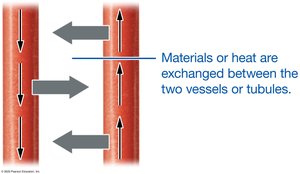
The Countercurrent Mechanism
Countercurrent Multiplier: In juxtamedullary nephrons, establishes medullary osmotic gradient by active NaCl transport in the ascending limb and water reabsorption in the descending limb.
Urea Recycling: Urea diffuses into the interstitial fluid, contributing to the gradient.
Countercurrent Exchanger: Vasa recta maintains the gradient by exchanging water and solutes without dissipating the gradient.


Urine Composition and Elimination
Urine Composition and Urinalysis
Normal urine contains water, electrolytes, and metabolic wastes (urea, creatinine, ammonia, uric acid).
Urinalysis examines color, translucency, odor, pH, specific gravity, and presence of abnormal solutes (e.g., blood, protein, glucose).
Renal Clearance
Measures the rate at which kidneys remove a substance from blood (mL/min).
Creatinine and inulin are used to estimate GFR; inulin is ideal as it is filtered but not reabsorbed or secreted.
Urine Transport, Storage, and Elimination
Urine drains from papillary ducts to minor calyces, major calyces, renal pelvis, ureters, bladder, and urethra.
Micturition: Reflex mediated by the parasympathetic nervous system; voluntary control develops with age.
Clinical Connections
Nephrolithiasis (Kidney Stones)
Crystalline structures (mainly calcium oxalate) form in the tubules; risk factors include dehydration, diet, and obesity.
Symptoms: Severe pain, hematuria, nausea, vomiting.
Diagnosis: Intravenous pyelogram (IVP).


Glomerulonephritis
Inflammation and damage to glomeruli; filtration membrane becomes leaky, leading to proteinuria and hematuria.
Can progress to renal failure if untreated.

Renal Failure
Acute: Sudden, often reversible.
Chronic: Progressive, often due to diabetes or hypertension; may require dialysis.
Dialysis: Hemodialysis or peritoneal dialysis removes wastes and balances fluids/electrolytes.
Diuretics
Loop Diuretics: Inhibit Na+/K+/2Cl- symporter in ascending limb; potassium-wasting.
Thiazide Diuretics: Block Na+/Cl- transporter in distal tubule.
Potassium-Sparing Diuretics: Block aldosterone or Na+ channels; prevent K+ loss.

Syndrome of Inappropriate ADH Secretion (SIADH)
Excess ADH causes water retention, low plasma osmolarity, and concentrated urine.
May be due to tumors or other causes.

Summary Table: Control of Glomerular Filtration Rate
Stimulus | Responding Mechanism | Main Effect(s) | Effect on GFR |
|---|---|---|---|
Increased afferent arteriole stretch | Myogenic | Vasoconstriction of afferent arteriole | Decrease |
Increased NaCl at macula densa | Tubuloglomerular feedback | Vasoconstriction of afferent arteriole | Decrease |
Decreased systemic blood pressure | RAAS | Vasoconstriction of efferent arteriole, systemic vasoconstriction, aldosterone/ADH release | Increase/maintain |
Increased blood volume | ANP | Dilation of afferent, constriction of efferent arteriole | Increase |
Sympathetic stimulation | Neural | Vasoconstriction, RAAS activation | Decrease (high), maintain (low) |
