 Back
BackThe Urinary System: Water Balance, Regulation, and Disorders
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
The Urinary System: Water Balance, Regulation, and Disorders
Water Reabsorption in the Nephron
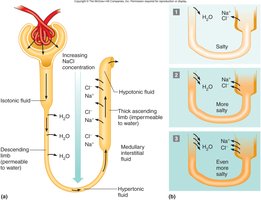
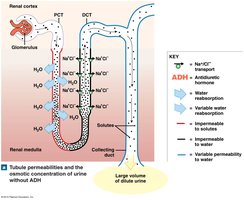
Water reabsorption is a critical process in the nephron, allowing the body to maintain fluid and electrolyte balance. The movement of water depends on the osmotic gradients established by solute reabsorption and the permeability of nephron segments.
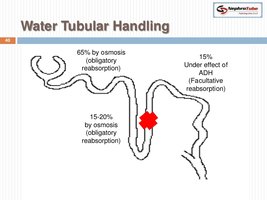
Obligatory Water Reabsorption: This is water movement that cannot be prevented and usually recovers about 85% of the filtrate produced. It occurs mainly in the proximal convoluted tubule (PCT) and descending limb of the nephron loop, where water follows solutes by osmosis.
Facultative Water Reabsorption: This process controls the volume of water reabsorbed along the distal convoluted tubule (DCT) and collecting duct. It accounts for about 15% of filtrate volume and is regulated by antidiuretic hormone (ADH), which increases water permeability in these segments.
Osmotic Gradient: The peritubular fluid, especially in the medulla, is hypertonic, creating ideal conditions for water reabsorption if the tubule is permeable to water.
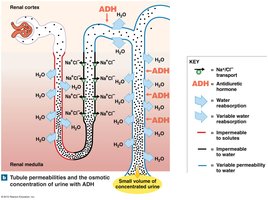
Role of Antidiuretic Hormone (ADH)
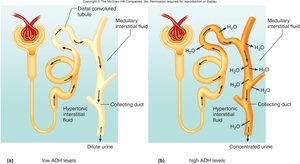
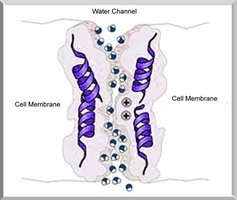
ADH is a hormone that regulates facultative water reabsorption by increasing the permeability of the collecting duct and late DCT to water. It does so by stimulating the insertion of aquaporin-2 water channels into the membranes of principal cells.
High ADH Levels: Kidneys produce concentrated urine and conserve water. Large volumes of water are reabsorbed, and urine solute concentration is high.
Low ADH Levels: Kidneys produce dilute urine, excreting excess water. Renal tubules reabsorb more solutes than water.
Regulation: ADH secretion increases when plasma osmolarity rises, enhancing water reabsorption to restore osmotic balance.

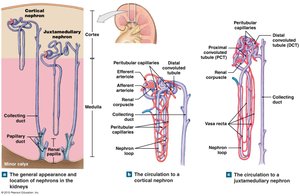
Juxtamedullary Nephrons and the Vasa Recta
Juxtamedullary nephrons have long loops that extend deep into the medulla and are essential for concentrating urine. The vasa recta, a network of capillaries, helps maintain the osmotic gradient in the medulla by countercurrent exchange, allowing solutes and water to be exchanged without disrupting the gradient.
Countercurrent Mechanism: Blood flows in opposite directions in the vasa recta and nephron loop, preserving the medullary gradient.
Importance: This mechanism allows mammals, birds, and some insects to produce highly concentrated urine, an adaptation crucial for terrestrial life.

Production of Dilute and Concentrated Urine
The kidneys adjust urine concentration and volume to maintain homeostasis. When water intake is high, dilute urine is produced; when dehydrated, urine becomes concentrated.
Minimum Urine Output: The kidney can produce as little as 400–500 mL of very concentrated urine per day, depending on the medullary osmotic gradient.
Adaptations: Desert mammals have extremely long nephron loops, allowing them to concentrate urine to a remarkable degree.
Disorders Affecting Water Balance
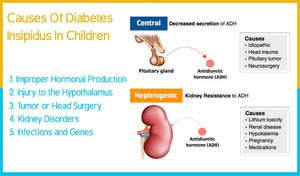
Diabetes Insipidus
Diabetes insipidus is characterized by excessive urination and thirst due to inadequate ADH production or renal insensitivity to ADH. This leads to the inability to concentrate urine, resulting in large volumes of dilute urine.
Diuretics
Diuretics are substances that increase urine flow by inhibiting water reabsorption at various points in the nephron. They are used clinically to manage hypertension, edema, and certain kidney disorders.
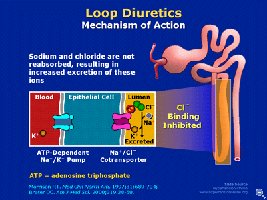
Types: Loop diuretics (e.g., furosemide) are the most potent, acting on the thick ascending limb of the nephron loop. Others include thiazides and potassium-sparing diuretics.
Mechanisms: Caffeine inhibits Na+ reabsorption, alcohol inhibits ADH secretion, and prescription diuretics act on different nephron segments.
Evaluation of Kidney Function
Kidney function is assessed using blood and urine tests. Key tests include:
Blood Urea Nitrogen (BUN): Measures nitrogen in blood from urea, indicating renal function.
Plasma Creatinine: Used to estimate glomerular filtration rate (GFR).
Renal Plasma Clearance: Indicates how effectively kidneys remove substances from plasma. Inulin clearance measures GFR; para-aminohippuric acid clearance measures renal plasma flow.
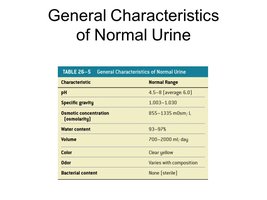
Urinalysis
Urinalysis examines the physical, chemical, and microscopic properties of urine, providing insights into body health and kidney function.
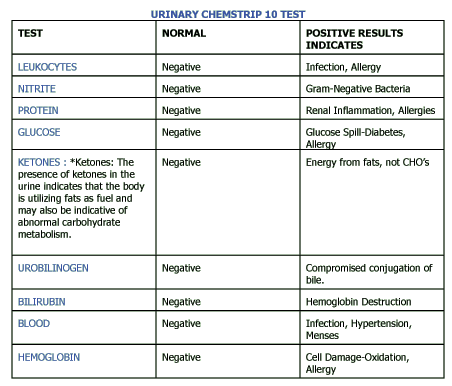
Test | Normal | Positive Results Indicate |
|---|---|---|
Leukocytes | Negative | Infection, Allergy |
Nitrite | Negative | Gram-Negative Bacteria |
Protein | Negative | Renal Inflammation, Allergies |
Glucose | Negative | Glucose Spill—Diabetes, Allergy |
Ketones | Negative | Energy from fats, not CHOs; abnormal metabolism |
Urobilinogen | Negative | Compromised conjugation of bile |
Bilirubin | Negative | Hemoglobin Destruction |
Blood | Negative | Infection, Hypertension, Menses |
Hemoglobin | Negative | Cell Damage, Oxidation, Allergy |
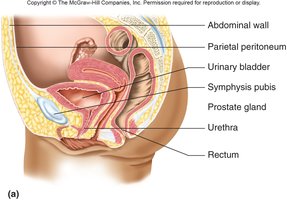
Urine Storage, Transportation, and Elimination
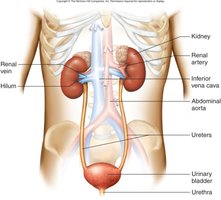
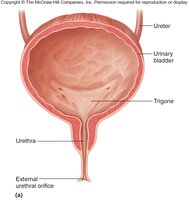
Urine is transported from the kidneys to the bladder via the ureters, stored in the bladder, and eliminated through the urethra. The process involves several anatomical structures and reflexes.
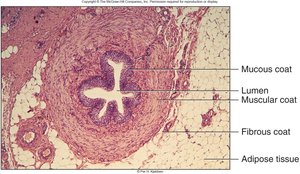
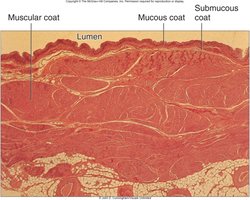
Ureters: Muscular tubes that transport urine by peristalsis, hydrostatic pressure, and gravity. They are retroperitoneal and have mucosa, muscularis, and fibrous coat layers.
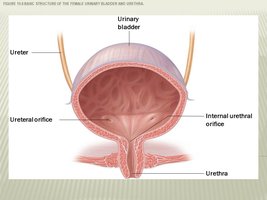
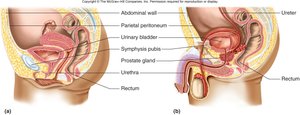
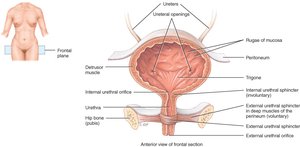
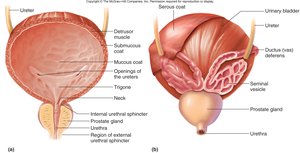
Urinary Bladder: A hollow, distensible organ with a capacity of 700–800 mL. It has four layers: mucosa (transitional epithelium), submucosa, muscularis (detrusor muscle), and adventitia/serosa.
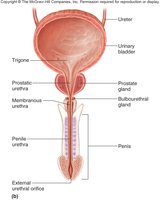
Trigone: A triangular area in the bladder floor defined by the openings of the ureters and urethra.
Urethra: Shorter in females (2.5–5 cm) and longer in males (19.5 cm), with different regions and sphincters for each sex.
Aging and the Urinary System
With aging, kidney function declines due to anatomical and functional changes. The number of functional nephrons decreases, GFR is reduced, and sensitivity to ADH diminishes, increasing the risk of dehydration and incontinence.
Homeostatic Imbalances and Disorders
Renal Calculi (Kidney Stones): Crystals of salts can form stones, potentially blocking the ureter. Treatment may involve shock wave lithotripsy.
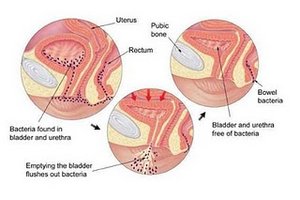
Urinary Tract Infections (UTIs): Infections can affect any part of the urinary system, including urethritis, cystitis, pyelonephritis, and pyelitis.
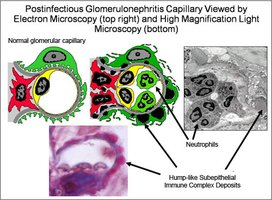
Glomerular Diseases: Glomerulonephritis is inflammation of the glomeruli, often following streptococcal infection, and can lead to renal failure.
Polycystic Kidney Disease: An inherited disorder causing cyst formation in the kidneys, leading to renal failure.
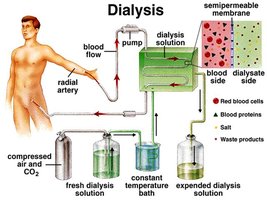
Chronic Renal Failure: Progressive, irreversible decline in GFR due to various causes, ultimately requiring dialysis or transplantation.

Additional info: The above notes integrate textbook-level explanations and context for each topic, ensuring a comprehensive and exam-ready review of the urinary system, its regulation, and associated disorders.
