 Back
BackChapter 1: Foundations of Medical Terminology and Medical Records
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Chapter 1: Introduction to Medical Terminology
Understanding Medical Terms: Word Structure
Medical terminology is built from word parts that convey specific meanings. Understanding how to break down and interpret these terms is essential for accurate communication in healthcare.
Word Root: The core of the word, indicating the main meaning. Some terms may have more than one root (e.g., osteoarthritis: osteo = bone, arthr = joint).
Prefix: Appears at the beginning of a word, often describing location, number, or time (e.g., peri- = around, as in pericardium).
Suffix: Added to the end of a word to indicate condition, disease, or procedure (e.g., -itis = inflammation, as in carditis).
Combining Vowel: Usually an 'o', used to link word roots or a root and suffix for easier pronunciation (e.g., cardiomyopathy).
Combining Form: The word root plus its combining vowel (e.g., bi/o = life, biology).
Rules for Combining Vowels:
Do not use a combining vowel if the suffix begins with a vowel (e.g., arthritis).
Use a combining vowel between two root words (e.g., gastroenteritis).
Common Combining Forms and Their Meanings
Cardi/o: heart (cardiac)
Dermat/o: skin (dermatology)
Gastr/o: stomach (gastric)
Hemat/o: blood (hematic)
Nephr/o: kidney (nephromegaly)
Ophthalm/o: eye (ophthalmic)
Ot/o: ear (otic)
Path/o: disease (pathology)
Pulmon/o: lung (pulmonary)
Rhin/o: nose (rhinoplasty)
Prefixes: Location, Number, and Time
Prefixes modify the meaning of the root word, often indicating location, number, or time.
a-, an-: without (aphasia, anoxia)
brady-: slow (bradycardia)
hyper-: excessive (hypertrophy)
hypo-: below, insufficient (hypodermic)
inter-: between (intervertebral)
intra-: within (intravenous)
pre-, post-: before, after (preoperative, postpartum)
bi-, tri-, quadri-: number prefixes (bilateral, triceps, quadriplegia)
Suffixes: Conditions, Diseases, Procedures
Suffixes are essential for specifying the nature of a medical term, such as a disease, condition, or procedure.
-algia, -dynia: pain (gastralgia, cardiodynia)
-itis: inflammation (dermatitis)
-oma: tumor, mass (carcinoma, hematoma)
-pathy: disease (myopathy)
-plasty: surgical repair (dermatoplasty)
-ectomy: surgical removal (gastrectomy)
-scopy: process of visually examining (gastroscopy)
Adjective Suffixes
Adjective suffixes convert word roots into adjectives, typically meaning "pertaining to."
-ac, -al, -an, -ar, -ary: pertaining to (cardiac, duodenal, ovarian, ventricular, pulmonary)
-ic, -ical, -ous, -tic: pertaining to (gastric, chemical, intravenous, acoustic)
Surgical and Procedural Suffixes
-centesis: puncture to withdraw fluid (arthrocentesis)
-ostomy: surgically create an opening (colostomy)
-otomy: cutting into (thoracotomy)
-tome: instrument to cut (dermatome)
-gram, -graphy: record, process of recording (electrocardiogram, electrocardiography)
-meter, -metry: instrument/process for measuring (audiometer, audiometry)
Singular and Plural Endings
Medical terms often have unique plural forms. Understanding these helps in interpreting medical records and literature.
Singular Ending | Example | Plural Ending | Example |
|---|---|---|---|
-a | vertebra | -ae | vertebrae |
-ax | thorax | -aces | thoraces |
-ex/-ix | appendix | -ices | appendices |
-is | metastasis | -es | metastases |
-ma | sarcoma | -mata | sarcomata |
-on | phalanx | -nges | phalanges |
-um | ovum | -a | ova |
-us | nucleus | -i | nuclei |
-y | biopsy | -ies | biopsies |
Medical Records: Components and Documentation
Purpose and Structure of the Medical Record
The medical record is a comprehensive chart documenting a patient's hospital stay, including daily condition, services received, and response to treatment. Each page must contain proper patient identification, such as name, date of birth, or medical record number.
Main Components of the Medical Record
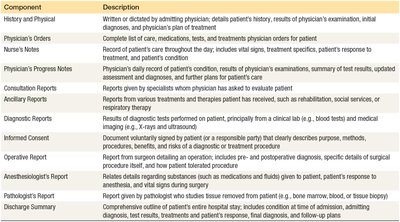
The following table summarizes the essential components and their descriptions:
Component | Description |
|---|---|
History and Physical | Written or dictated by admitting physician; details patient’s history, results of physician’s examination, initial diagnosis, and physician’s plan of treatment. |
Physician’s Orders | Complete list of care, medications, tests, and treatments physician orders for patient. |
Nurse’s Notes | Record of patient’s care throughout the day; includes vital signs, treatment specifics, patient’s response to treatment, and patient’s condition. |
Physician’s Progress Notes | Physician’s daily record of patient’s condition, results of physician’s examinations, summary of test results, updated assessment and diagnoses, and further plans for patient’s care. |
Consultation Reports | Reports given by specialists when physician has asked to evaluate patient. |
Ancillary Reports | Reports from various treatments and therapies patient has received, such as rehabilitation, social services, or respiratory therapy. |
Diagnostic Reports | Results of diagnostic tests performed on patient, principally from a clinical lab (e.g., blood tests) and medical imaging (e.g., X-rays). |
Informed Consent | Document voluntarily signed by patient or a responsible party that clearly describes purpose, methods, procedures, benefits, and risks of a diagnostic or treatment procedure. |
Operative Report | Report from surgeon detailing an operation; includes pre- and post-operative diagnoses, specific details of surgical procedure itself, and how patient tolerated procedure. |
Anesthesiologist’s Report | Relates details regarding substances given to patient, patient’s response to anesthesia, and vital signs during surgery. |
Psychologist’s Report | Includes assessment of patient’s mental status, including behavioral observations and results of psychological tests. |
Discharge Summary | Comprehensive outline of patient’s entire hospital stay; includes condition at time of admission, admitting diagnosis, test results, treatments and patient’s response, final diagnosis, and follow-up plans. |
Example: Use of Medical Terminology in Records
When documenting a patient with carditis (inflammation of the heart), the medical record will include the term in the physician’s notes, diagnostic reports, and possibly in the discharge summary. Accurate use of prefixes, suffixes, and combining forms ensures clarity and precision in patient care.
