 Back
BackOxygen Therapy and Airway Management: Medical Terminology Study Notes
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Oxygen Therapy
Introduction to Oxygen Therapy
Oxygen therapy is a critical intervention in medical care, used to treat hypoxaemia (low blood oxygen levels). Oxygen is delivered from wall taps at 100% concentration and is administered to patients using various devices that adjust the concentration and flow rate of inspired oxygen.
Oxygen Concentration: The percentage of oxygen a patient receives depends on the flow rate and the delivery device.
Flow Rate: Adjustable from 0–15 L/min at the wall tap.
Prescription: Oxygen is a prescription-only medicine (POM) and must be prescribed with a target saturation range.
Indication: Oxygen treats hypoxaemia, not breathlessness in non-hypoxaemic patients.
Assessment and Monitoring
Oxygen therapy should be guided by regular assessment and monitoring of oxygen saturation using pulse oximetry, which is considered the 'fifth vital sign' alongside pulse, blood pressure, temperature, and respiratory rate.
Pulse Oximetry: Essential for all breathless and acutely ill patients; results should be recorded with the inspired oxygen concentration.
Target Saturation: Most acutely ill patients: 94–98%. Patients at risk of hypercapnic respiratory failure: 88–92% or patient-specific range.
Clinical Assessment: Required if saturation falls by ≥3% or below the target range.
Early Warning Scores: Use systems like NEWS for ongoing assessment outside critical care areas.
Oxygen Delivery Devices
Different devices are used to deliver oxygen, each with specific indications, flow rates, and oxygen concentrations.
Nasal Cannula
Oxygen Delivery: 24–30% O2
Flow Rate: 1–4 L/min (2 L/min is most comfortable; >4 L/min may dry the nose)
Indication: Non-acute or mildly hypoxic patients

Simple Face Mask (Hudson Mask)
Oxygen Delivery: 30–40% O2
Flow Rate: 5–10 L/min
Indication: Mild to moderate hypoxia
Limitations: Less precise FiO2 control; aspiration risk if vomiting occurs
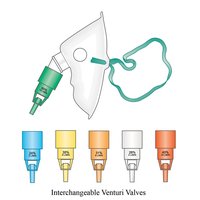
Venturi Mask
Venturi masks deliver precise oxygen concentrations and are especially important in patients with COPD to avoid over-oxygenation.
Oxygen Delivery: 24–60% O2 (depending on valve color)
Flow Rate: Varies by color (e.g., Blue: 2–4 L/min = 24%, White: 4–6 L/min = 28%, Yellow: 8–10 L/min = 35%, Red: 10–12 L/min = 40%, Green: 12–15 L/min = 60%)
Non-Rebreather Mask
Oxygen Delivery: 85–90% O2
Flow Rate: 15 L/min
Indication: Acutely unwell patients requiring high concentrations of oxygen
Precaution: Do not maintain 15 L/min for prolonged periods; avoid saturations of 100%

Humidified Oxygen
Purpose: Prevents drying of mucous membranes and airway damage
Mechanism: Oxygen is passed through a humidifying device to produce sterile vapor
Issues: Water can pool in tubing, potentially obstructing flow
Non-Invasive Ventilation (CPAP/BiPAP)
CPAP: Continuous positive airway pressure; used in acute pulmonary oedema and sleep apnoea
BiPAP: Bilevel positive airway pressure; used in COPD exacerbations
Invasive Ventilation
Oxygen Delivery: Up to 100% O2
Indication: Intensive care and surgical settings
Mechanism: Artificial airway with ventilation bag or machine
Oxygen Administration and Monitoring
Oxygen should be administered by trained staff using appropriate devices and flow rates.
Oxygen saturation and delivery system (including flow rate) must be recorded on the patient's chart.
Adjustments should be made to maintain target saturation; prompt assessment is needed if saturation falls.
Oxygen should be weaned and discontinued when the patient can maintain target saturation on room air, but the prescription should remain in case of deterioration.
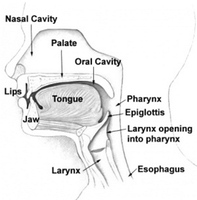
Airway Management
Introduction to Airway Management
Airway management is essential for ensuring adequate ventilation and oxygenation in patients with compromised airways. It involves recognizing airway obstruction, performing simple maneuvers, and using adjuncts to maintain patency.
Causes of Airway Obstruction
Tongue: Most common cause in unconscious patients (relaxes and falls back)
Foreign bodies: Vomit, blood, secretions, or external objects
Swelling: Allergic reactions, trauma, or infection

Identifying Airway Compromise
Conscious Patient: Look for signs such as stridor, use of accessory muscles, inability to speak, or cyanosis.
Unconscious Patient: Assess for absent or abnormal breathing, snoring, or gurgling sounds.
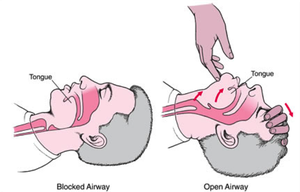
Simple Airway Manoeuvres
Basic techniques can relieve airway obstruction caused by the tongue or soft tissues.
Head Tilt, Chin Lift: Tilts the head back and lifts the chin to open the airway.
Jaw Thrust: Used if cervical spine injury is suspected; lifts the jaw forward without moving the neck.
Suction: Removes secretions, vomit, or blood from the airway.


Simple Airway Adjuncts
Nasopharyngeal Airway (NPA): Soft tube inserted through the nostril to maintain airway patency. Size is marked on the tube (6 mm for women, 7 mm for men). Lubricate before insertion and aim towards the occiput.
Oropharyngeal Airway (OPA): Curved device inserted into the mouth to prevent the tongue from obstructing the airway. Measure from incisors to the angle of the jaw; insert upside down and rotate 180° behind the tongue.
Advanced Airway Devices
I-gel: Supraglottic airway device inserted into the mouth, gliding along the hard palate until resistance is felt. Used when basic maneuvers and adjuncts are insufficient.
Summary Table: Oxygen Delivery Devices
Device | Oxygen Concentration (%) | Flow Rate (L/min) | Indication |
|---|---|---|---|
Nasal Cannula | 24–30 | 1–4 | Mild hypoxia, non-acute |
Simple Face Mask | 30–40 | 5–10 | Mild to moderate hypoxia |
Venturi Mask | 24–60 | 2–15 (varies by valve) | COPD, precise FiO2 needed |
Non-Rebreather Mask | 85–90 | 15 | Severe hypoxia, emergencies |
