 Back
BackImmunodeficiencies, Transplantation, and HIV/AIDS: Microbiology Study Notes
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Transplantation and Immune Response
Types of Grafts
Transplantation involves moving tissue from one individual to another. The immune system plays a critical role in determining the success of these procedures.
Autograft: Transplantation of tissue within the same individual (e.g., skin grafts).
Isograft: Transplantation between genetically identical individuals (e.g., identical twins).
Allograft: Transplantation between genetically different members of the same species.
Xenotransplantation product: Transplantation using tissue from a different species (e.g., pig heart valves in humans). These require overcoming hyperacute rejection due to nonhuman antigens.
Graft-versus-host (GVH) disease: Occurs when transplanted immunocompetent cells (such as B and T cells from bone marrow) attack the recipient's tissues.
Immunosuppression in Transplantation
To prevent rejection of transplanted tissue, immunosuppressive drugs are used. These drugs primarily suppress cell-mediated immunity, allowing humoral immunity to remain functional so the patient can still fight off infections. However, immunosuppression increases susceptibility to infections and certain cancers.
The Immune System and Cancer
Immune Surveillance and Cancer
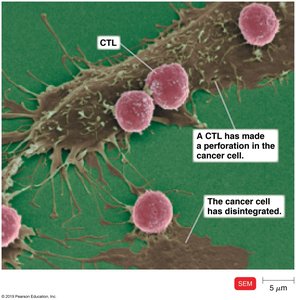
Cancer cells are mutated normal cells that divide uncontrollably. The immune system, particularly cytotoxic T lymphocytes (CTLs) and macrophages, can recognize and destroy many cancer cells through a process called immune surveillance. However, cancer cells may evade detection by lacking recognizable antigens or by mutating rapidly.
Tumor-associated antigens: Unique or abnormally expressed proteins on cancer cells that can be targeted by the immune system.
CTLs: Activated cytotoxic T cells that can lyse cancer cells.
Immunotherapy for Cancer
Immunotherapy leverages the immune system to treat cancer. Approaches include:
Vaccines: Used for prevention (e.g., HPV vaccine for cervical cancer, hepatitis B vaccine for liver cancer).
Monoclonal antibodies (Mabs): Engineered antibodies that target specific cancer cell antigens (e.g., Herceptin for breast cancer).
Immunotoxins: Monoclonal antibodies linked to toxic agents, which specifically target and kill cancer cells without harming normal cells.
Human Microbiome and Inflammatory Bowel Disease (IBD)
Role of the Microbiome
The human microbiome is essential for the proper development and function of the immune system. Increased diversity in the microbiome is associated with better health, as described by the hygiene hypothesis.
Dysbiosis: An imbalance in the microbiome that can lead to adverse health effects, such as the proliferation of Clostridium difficile after antibiotic therapy.
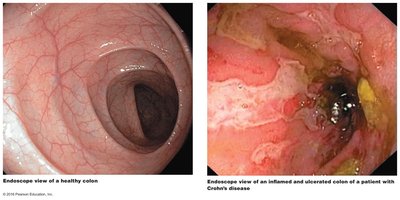
IBDs: Conditions like ulcerative colitis and Crohn's disease may be linked to dysbiosis.
Treatments for IBD
Fecal transplants: Transferring gut microbiota from a healthy donor to a patient to restore microbial balance.
Helminth therapy: Using whipworm eggs (from pigs) to suppress T helper cell pathways and reduce inflammation in Crohn's disease.
Immunodeficiencies
Types of Immunodeficiencies
Immunodeficiencies are conditions where the immune system's ability to fight infections is compromised.
Congenital immunodeficiencies: Caused by genetic defects (e.g., DiGeorge syndrome, where patients lack a thymus and thus cell-mediated immunity).
Acquired immunodeficiencies: Develop during life due to drugs, cancers, or infections (e.g., AIDS).
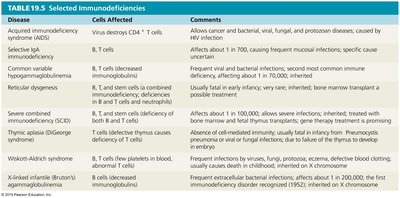
Selected Immunodeficiencies
Disease | Cells Affected | Comments |
|---|---|---|
Acquired immunodeficiency syndrome (AIDS) | Virus destroys CD4+ T cells | Allows cancer and bacterial, viral, fungal, and protozoan diseases; caused by HIV infection |
Selective IgA deficiency | B, T cells | Affects about 1 in 700; causes frequent mucosal infections |
Common variable hypogammaglobulinemia | B, T cells | Frequent viral and bacterial infections; most common immune deficiency, affecting about 1 in 70,000 |
Reticular dysgenesis | B and T cells, or deficiency of stem cells | Usually fatal in early infancy; very rare; inherited; more common after transplant |
Severe combined immunodeficiency (SCID) | B and T cells, or deficiency of stem cells | Affects about 1 in 100,000; allows severe infections; inherited; treated with bone marrow or stem cell transplants |
Thymic aplasia (DiGeorge syndrome) | Defective thymus causes deficiency of T cells | Absence of cell-mediated immunity; usually fatal in infancy; Pneumocystis infection or viral/fungal infections due to lack of thymus to educate T cells |
Wiskott-Aldrich syndrome | T cells (few platelets in blood, usually eczema) | Frequent infections by viruses, fungi, or bacteria; eczema; defective blood clotting; usually causes childhood death; inherited, on X chromosome |
X-linked agammaglobulinemia (Bruton's) | B cells | Frequent extracellular bacterial infections; affects about 1 in 200,000; the first immunodeficiency disorder recognized (1952); inherited, on X chromosome |
Acquired Immunodeficiency Syndrome (AIDS) and HIV
Discovery and Origin of AIDS
AIDS was first recognized in 1981 in the United States, with clusters of unusual infections and cancers in young men. In 1983, HIV was identified as the causative agent. HIV likely originated from simian immunodeficiency virus (SIV) crossing into humans in Africa around 1908, spreading due to urbanization and increased sexual activity.
Structure of HIV
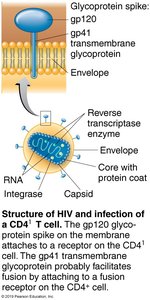
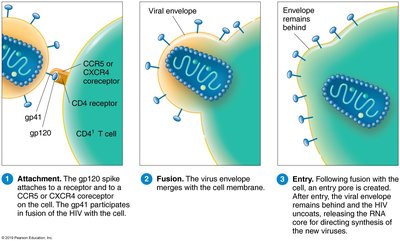
HIV is a retrovirus of the genus Lentivirus. It contains two identical strands of RNA, the enzyme reverse transcriptase, and a phospholipid envelope with glycoprotein spikes (gp120 and gp41).
gp120: Surface glycoprotein that binds to CD4 receptors on host cells.
gp41: Transmembrane glycoprotein involved in fusion of the virus with the host cell membrane.
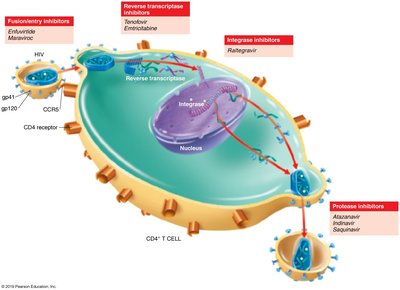
HIV Entry and Replication
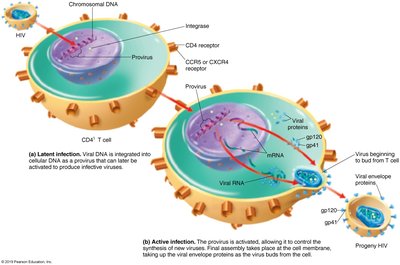
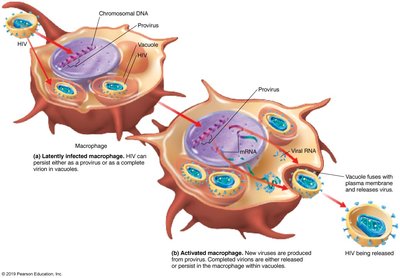
HIV infects cells by binding to CD4 receptors and coreceptors (CCR5 or CXCR4) on T helper cells, macrophages, and dendritic cells. The virus fuses with the cell membrane, and its RNA is reverse transcribed into DNA, which integrates into the host genome.
Active infection: New viruses are produced and bud from the host cell.
Latent infection: Viral DNA remains integrated in the host genome as a provirus, sometimes in memory T cells, serving as a reservoir for HIV.
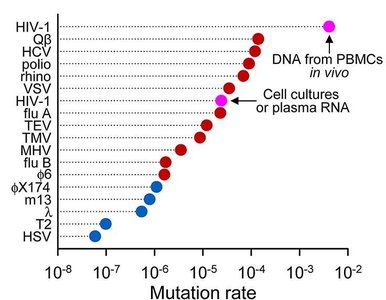
HIV Mutation and Immune Evasion
HIV has a high mutation rate due to the lack of proofreading by reverse transcriptase. This leads to rapid antigenic changes, making it difficult for the immune system to control the virus and for vaccines to be effective.
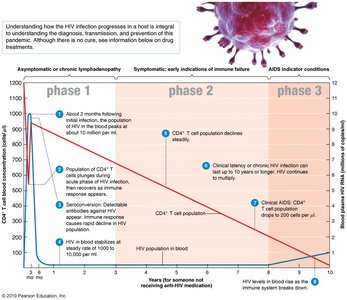
Stages of HIV Infection
Phase 1: Asymptomatic or chronic lymphadenopathy; high viral load and rapid loss of CD4+ T cells.
Phase 2: Steady decline in CD4+ T cells; persistent infections and mild symptoms.
Phase 3 (AIDS): CD4+ T cell count drops below 200 cells/μl; severe opportunistic infections and cancers occur.
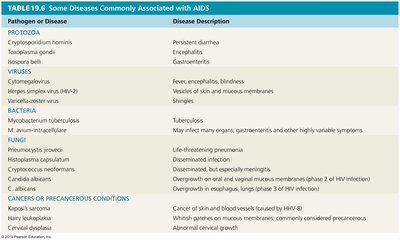
Opportunistic Infections and Cancers in AIDS
As the immune system fails, patients become susceptible to a wide range of infections and cancers.
Pathogen or Disease | Disease Description |
|---|---|
Cryptosporidium hominis | Persistent diarrhea |
Toxoplasma gondii | Encephalitis |
Herpes simplex virus (HSV-2) | Vesicles of skin and mucous membranes |
Mycobacterium tuberculosis | Tuberculosis |
Pneumocystis jirovecii | Life-threatening pneumonia |
Kaposi's sarcoma | Cancer of skin and blood vessels (caused by HHV-8) |


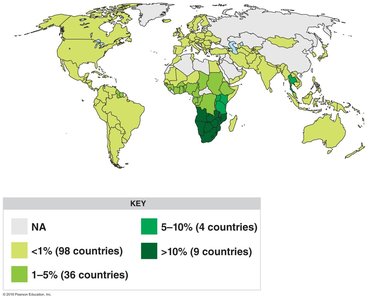
HIV Transmission and Epidemiology
HIV is transmitted through intimate sexual contact, blood, contaminated needles, organ transplants, and from mother to child. The virus survives for hours outside a cell and for days inside cells. Prevention includes safe sex practices, sterile needles, and antiretroviral therapy.
Prevention and Treatment of HIV/AIDS
Antiretroviral therapy (ART) targets different stages of the HIV life cycle, including entry, reverse transcription, integration, and protease activity. Universal precautions and education are essential for prevention.
Challenges in HIV Vaccine Development
Developing an HIV vaccine is challenging due to the lack of a natural model of immunity, the virus's rapid mutation rate, and its ability to hide within host cells.

