 Back
BackInfectious Diseases Affecting the Nervous System: Microbiology Study Notes
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Infectious Diseases Affecting the Nervous System
Overview
The nervous system can be affected by a variety of infectious agents, including bacteria, viruses, fungi, and protozoa. These infections can lead to severe and sometimes fatal diseases such as meningitis, encephalitis, meningoencephalitis, tetanus, and botulism. Understanding the causative agents, pathogenesis, clinical manifestations, diagnosis, treatment, and prevention is crucial for effective management and control.
Meningitis
Definition and General Features
Meningitis is the inflammation of the meninges, the protective membranes covering the brain and spinal cord.
It is an anatomical syndrome with similar symptoms regardless of the causative microorganism.
Acute bacterial meningitis is more severe than viral or fungal forms.
Diagnosis involves lumbar puncture, Gram stain, and/or culture of cerebrospinal fluid (CSF).
Immediate treatment with broad-spectrum antibiotics is critical.
Common Symptoms:
Severe headache
Painful or stiff neck
Fever
Nausea and vomiting
Photophobia (sensitivity to light)
Skin rashes (in specific types)
Increased white blood cells in CSF
Bacterial Meningitis: Neisseria meningitidis
Gram-negative diplococcus, known as the meningococcus.
Responsible for epidemic forms and the most serious cases of acute meningitis.
Most cases occur in young children; vaccination is recommended from age 11.
Serotypes B, C, and Y are most common.
Pathogenesis and Virulence Factors
Entry via upper respiratory tract, then bloodstream, then meninges.
Releases endotoxin, causing cytokine-mediated vascular damage, hemorrhage, and petechiae.
Produces IgA protease and a capsule to evade immune defenses.
Clinical Manifestations
Sudden onset, high fever (>40°C), sore throat, chills, delirium, widespread bleeding, shock, coma, cardiac failure, adrenal damage, and rapid death.
Transmission and Epidemiology
Spread by close contact with respiratory secretions or droplets.
Reservoir: human nasopharynx; highest risk in children, adolescents, and young adults in close quarters.
Diagnosis and Treatment
Medical emergency; rapid Gram stain and oxidase testing of CSF, blood, or nasopharyngeal samples.
Culture on modified Thayer-Martin or chocolate agar in high CO2.
Immediate high-dose intravenous penicillin G; preventive therapy for contacts with rifampin or tetracycline.
Bacterial Meningitis: Streptococcus pneumoniae
Gram-positive, flattened coccus (pneumococcus), appears in pairs.
Most frequent cause of community-acquired meningitis and bacterial pneumonia.
Virulence: polysaccharide capsule, alpha-hemolysin, hydrogen peroxide, induces apoptosis in brain cells.
Often resistant to penicillin; initial therapy is vancomycin + ceftriaxone.
Vaccines: Prevnar (children), Pneumovax 23 (adults).
Bacterial Meningitis: Haemophilus influenzae
Severe form, mostly nonserotype B strains in the U.S.
Incidence greatly reduced by vaccination; still common globally in children under 5.
Bacterial Meningitis: Listeria monocytogenes
Gram-positive, variable morphology, no capsule or endospores, motile with flagella.
Resistant to cold, heat, salt, pH extremes, and bile; grows inside host cells and spreads cell-to-cell.

Mild in healthy adults; severe in elderly, immunocompromised, fetuses, and neonates (30% mortality).
Transmitted via contaminated dairy, poultry, and meat; diagnosed by cold enrichment and rapid kits.
Treated with ampicillin and trimethoprim-sulfamethoxazole; prevention by food safety and avoiding unpasteurized cheeses in pregnancy.
Fungal Meningitis: Cryptococcus neoformans
Encapsulated yeast, causes chronic or acute meningoencephalitis, especially in AIDS patients.
Primary reservoir: bird droppings, especially pigeons; inhaled yeast cells cause infection.
Highest risk in immunocompromised; often fatal without treatment.

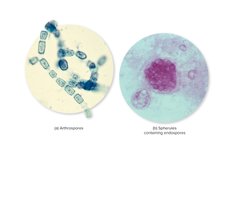
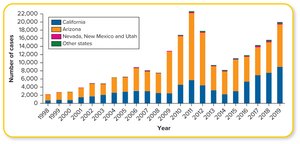
Fungal Meningitis: Coccidioides species
Dimorphic fungi causing "Valley Fever"; forms arthroconidia in soil and spherules in tissue.
Highly virulent; pulmonary infection can disseminate to meninges, bones, and skin.
Endemic in southwestern U.S., Mexico, Central and South America; outbreaks linked to soil disruption.
Viral (Aseptic) Meningitis
Most common form; 90% caused by enteroviruses, especially in children.
Symptoms are milder than bacterial or fungal meningitis; usually self-limited within 2 weeks.
Diagnosis by exclusion of bacteria/fungi/protozoa in CSF; confirmed by viral culture or antigen tests.
Treatment is supportive; mortality <1%.
Neonatal Meningitis
Transmitted from mother in utero or during birth; increased risk in premature infants.
Common agents: Streptococcus agalactiae (Group B strep), Escherichia coli (K1 strain), Listeria monocytogenes, Cronobacter sakazakii.
Prevention: maternal screening, intrapartum antibiotics, safe feeding practices.
Poliomyelitis
Overview and Signs/Symptoms
Acute enteroviral infection of the spinal cord, causing neuromuscular paralysis.
Symptoms: mild viremia, fever, headache, nausea, sore throat, myalgia; can progress to flaccid paralysis, especially of limbs and respiratory muscles.
Bulbar polio affects brainstem, leading to respiratory failure.
Causative agent: Poliovirus (Picornaviridae, Enterovirus); nonenveloped, RNA virus, acid-stable.
Transmission: fecal-oral route via contaminated food, water, hands, or objects.
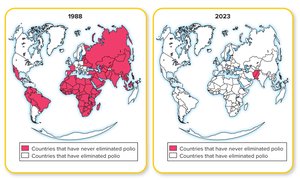
Prevention: vaccination (IPV and OPV); eradication efforts ongoing.
Meningoencephalitis
Naegleria fowleri
Free-living amoeba causing primary amoebic meningoencephalitis (PAM).
Infection via nasal passages during swimming in warm freshwater; rapid progression to brain destruction and death.
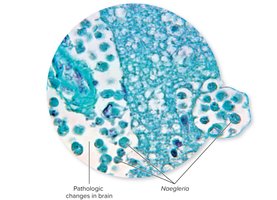
Prevention: proper chlorination of pools; treatment rarely successful.
Acanthamoeba
Causes granulomatous amoebic meningoencephalitis (GAM); slower progression than Naegleria.
Enters via broken skin, conjunctiva, or lungs; risk in contact lens wearers and immunocompromised.
Acute Encephalitis
General Features
Inflammation of the brain, usually viral (arboviruses, herpesviruses, JC virus).
Symptoms: behavior changes, confusion, seizures, decreased consciousness.
Diagnosis: patient history, serology, nucleic acid tests.
Treatment: empiric acyclovir for herpesvirus; supportive care for arboviral encephalitis.
Arboviral Encephalitis
Transmitted by mosquitoes; includes West Nile virus, equine encephalitis, etc.
Pathogenesis: virus replicates in lymphatic tissue, then invades brain causing inflammation and neurological damage.
Prevention: mosquito control; no specific antiviral treatment.
Tetanus
Overview and Pathogenesis
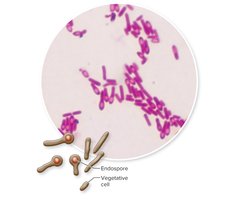
Neuromuscular disease caused by Clostridium tetani, a Gram-positive, endospore-forming anaerobe.
Endospores enter through wounds; vegetative cells produce tetanospasmin, a neurotoxin blocking inhibition of muscle contraction.
Symptoms: lockjaw (trismus), muscle rigidity, risus sardonicus, respiratory failure.

Transmission: puncture wounds, burns, umbilical stumps, IV drug use.
Prevention: vaccination (toxoid), TIG for exposed or unvaccinated individuals.
Treatment: TIG, penicillin G, muscle relaxants, supportive care.
Botulism
Overview and Pathogenesis
Caused by Clostridium botulinum exotoxin; associated with improperly preserved foods.
Botulinum toxin blocks acetylcholine release at neuromuscular junctions, causing flaccid paralysis.
Symptoms: double vision, dysphagia, dizziness, descending paralysis, respiratory failure.
Diagnosis: clinical suspicion, laboratory confirmation, notification of health authorities.
Treatment: antitoxin, respiratory and cardiac support; prevention by proper food handling.
Summary Table: Major Causes of Meningitis
Agent | Type | Key Features | Prevention/Treatment |
|---|---|---|---|
Neisseria meningitidis | Bacteria | Rapid onset, petechiae, epidemic potential | Vaccine, penicillin G, prophylaxis for contacts |
Streptococcus pneumoniae | Bacteria | Community-acquired, often penicillin-resistant | Vaccines, vancomycin + ceftriaxone |
Haemophilus influenzae | Bacteria | Severe in children, reduced by vaccine | Vaccine, antibiotics |
Listeria monocytogenes | Bacteria | Foodborne, affects neonates/elderly | Ampicillin, food safety |
Cryptococcus neoformans | Fungus | Chronic, AIDS-associated | Antifungals, avoid bird droppings |
Coccidioides spp. | Fungus | "Valley Fever", endemic in SW U.S. | Antifungals, avoid dust exposure |
Viruses (Enteroviruses, HSV-2) | Virus | Milder, self-limited | Supportive care |
Streptococcus agalactiae | Bacteria | Neonatal, from birth canal | Maternal screening, penicillin |
Escherichia coli (K1) | Bacteria | Neonatal, high mortality | IV antibiotics |
