 Back
BackInfectious Diseases Affecting the Skin and Eyes: Microbiology Study Notes
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Infectious Diseases Affecting the Skin and Eyes
Overview
Infectious diseases of the skin and eyes are caused by a variety of microorganisms, including bacteria, viruses, fungi, and protozoa. These infections can range from mild and self-limiting to severe and life-threatening, especially in immunocompromised individuals or neonates. Understanding the causative agents, pathogenesis, clinical manifestations, diagnosis, and treatment options is essential for effective management and prevention.
MRSA Skin and Soft-Tissue Infection
Characteristics and Epidemiology
MRSA (Methicillin-resistant Staphylococcus aureus) is a common cause of skin lesions in both community and healthcare settings.
Staphylococcus aureus is a Gram-positive coccus that grows in clusters and is nonmotile.
It is highly resistant to multiple antibiotics and can survive harsh environmental conditions (high salt, pH extremes, high temperatures, air drying).
Approximately one-third of the population carries S. aureus as normal skin biota.
Clinical Presentation
Lesions are raised, red, tender, and localized, often containing pus and feeling hot to the touch.
Lesions frequently occur at sites of skin breaks or around hair follicles.
Fever is a common systemic symptom.

Transmission and Prevention
MRSA can contaminate various surfaces (e.g., gym equipment, razors, electronic devices).
Active lesions should be covered to prevent transmission.
Good hygiene is the primary preventive measure.
Pathogenesis and Diagnosis
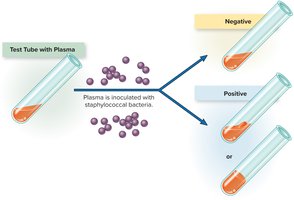
Virulence factors include coagulase (diagnostic), hyaluronidase, staphylokinase, DNase, and lipase.
Diagnosis involves PCR, culture on blood agar or mannitol salt agar, catalase test, and coagulase test.

Treatment
Incision and drainage of lesions are often required.
Antimicrobial therapy should include more than one antibiotic; vancomycin is commonly recommended in the U.S.
Maculopapular Rash Diseases
Overview
Maculopapular rash diseases are characterized by flat or slightly raised colored bumps. Common causes include measles, rubella, fifth disease, and roseola.
Measles (Rubeola)
Highly contagious viral disease with significant morbidity and mortality before widespread vaccination.
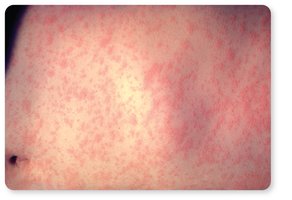
Symptoms: sore throat, dry cough, headache, conjunctivitis, lymphadenitis, fever, Koplik’s spots (oral lesions), and a red maculopapular rash starting on the head and spreading to the trunk and extremities.
Complications: laryngitis, bronchopneumonia, secondary bacterial infections, encephalitis, and subacute sclerosing panencephalitis (rare, progressive neurological degeneration).
Pathogenesis: Virus implants on respiratory mucosa, spreads via lymphatics and bloodstream, forms syncytia (giant cells).
Diagnosis: Clinical presentation, ELISA for IgM antibodies.
Prevention: MMR vaccine (live, attenuated virus).
Treatment: Supportive care, vitamin A supplementation.
Rubella (German Measles)
Generally a mild rash disease, but can cause severe congenital defects if contracted during pregnancy.
Symptoms: Pink macules and papules, joint inflammation in adults.
Congenital rubella: teratogenic, causing deafness, cardiac and ocular defects, and mental retardation.
Causative agent: Rubivirus (Togaviridae).
Diagnosis: IgM antibody detection (ELISA or latex agglutination).
Prevention: MMR vaccine; no specific treatment for congenital cases.
Fifth Disease (Erythema Infectiosum)
Caused by Parvovirus B19.
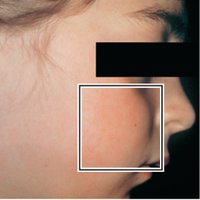
Symptoms: "Slapped cheek" rash, spreading to arms, legs, and trunk; rash may recur with heat or activity.
Diagnosis: Clinical presentation, rule out rubella by IgM testing.
No vaccine or specific treatment; disease is usually mild.
Roseola (Sixth Disease)
Common in young children; caused by Human herpesvirus 6 (HHV-6).
Symptoms: High fever (may cause seizures), followed by a maculopapular rash as fever subsides.
Diagnosis: Clinical presentation.
No vaccine or specific treatment; infection is nearly universal by adulthood.

Impetigo
Characteristics and Causative Agents
Superficial bacterial infection causing flaking or peeling skin, often with honey-colored crusts.
Caused by Staphylococcus aureus and/or Streptococcus pyogenes.
S. pyogenes often initiates infection; S. aureus may take over later.
S. aureus produces exfoliative toxins A and B, causing blistering.
S. pyogenes is beta-hemolytic and can cause a range of other diseases (pharyngitis, scarlet fever, etc.).
Impetigo in newborns is more often caused by S. pyogenes; in older children, S. aureus is more common.
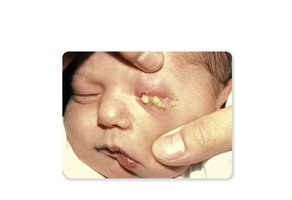
Staphylococcal Scalded Skin Syndrome (SSSS)
Overview
Dermolytic condition caused by S. aureus, primarily affecting newborns and infants.
Phage-encoded exfoliative toxins cause widespread desquamation (peeling) of the skin.
Bullous lesions appear, often around the umbilical area or in the diaper/axilla region.

Diagnosis is clinical; immediate systemic antibiotics are required.
Prevention includes eliminating carriers among caregivers.
Vesicular or Pustular Rash Diseases
Chickenpox (Varicella)
Caused by Human herpesvirus 3 (HHV-3, varicella-zoster virus).
Symptoms: Fever, centripetal rash (more lesions on trunk), lesions progress from macules to vesicles, then crust over.
Highly contagious; transmitted via respiratory droplets and lesion fluid.
Prevention: Varivax vaccine; ProQuad for MMRV.
Treatment: Supportive; acyclovir for at-risk patients.
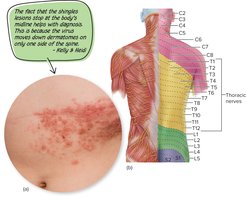
Shingles (Herpes Zoster)
Reactivation of latent HHV-3 in sensory ganglia, causing painful, asymmetrical vesicular rash.
Postherpetic neuralgia may cause prolonged pain.
Prevention: Shingrix vaccine for adults over 50.
Smallpox
Caused by Variola virus (Orthopoxvirus).
Symptoms: Fever, malaise, rash progressing from macules to pustules, scarring.
Highly virulent (variola major) or milder (variola minor).
Eradicated globally by vaccination; now a bioterrorism concern.
Treatment: Tecovirimat and cidofovir (FDA-approved).

Large Pustular Skin Lesions
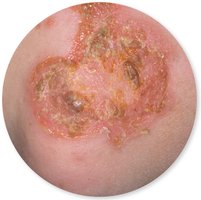
Leishmaniasis
Cutaneous leishmaniasis: localized skin infection; mucocutaneous form affects mucous membranes.
Causative agents: Leishmania tropica (cutaneous), L. brasiliensis (mucocutaneous).
Transmitted by female sand flies; endemic in equatorial regions.
Diagnosis: Microscopic visualization.
No vaccine; prevention is by avoiding sand fly bites.
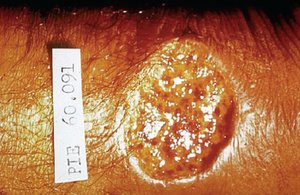
Cutaneous Anthrax
Caused by Bacillus anthracis.
Symptoms: Papule becomes necrotic, ruptures to form a painless black eschar.
Transmission: Endospores enter through skin cuts or abrasions; can be occupational or bioterrorism-related.
Diagnosis: Culture, serology, PCR.
Vaccine for high-risk groups; untreated cases can be fatal.

Cutaneous and Superficial Mycoses (Ringworm and Tinea Versicolor)
Ringworm (Dermatophytosis)
Caused by dermatophytes: Trichophyton, Microsporum, Epidermophyton.
Confined to nonliving epidermal tissues, hair, and nails.
Transmission: Direct or indirect contact with infected humans or animals.
Treatment: Topical antifungal ointments; some drugs accelerate skin shedding.







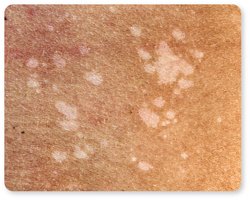
Superficial Mycoses (Tinea Versicolor)
Caused by Malassezia species (yeast).
Involves the outer epidermal surface; primarily cosmetic effects.
Nearly all humans are colonized by Malassezia.

Conjunctivitis (Pinkeye)
Overview and Clinical Features
Infection of the conjunctiva, common in all age groups.
Bacterial infections: milky discharge; viral infections: clear, watery exudate.
Highly contagious; can be caused by bacteria, viruses, or allergens.
Causative Agents and Transmission
Neonatal conjunctivitis: Neisseria gonorrhoeae, Chlamydia trachomatis (vertical transmission from mother).
Other bacteria: Staphylococcus epidermidis, S. aureus, Streptococcus pneumoniae, Haemophilus influenzae, Moraxella.
Viral: Adenoviruses are common causes.
Prevention and Treatment
Ciprofloxacin eye drops are commonly used for bacterial cases.
Prophylactic antibiotics may be prescribed even if viral infection is suspected.
Persistent symptoms warrant further diagnostic evaluation.
Keratitis
Overview
Infection of the cornea, potentially leading to blindness.
Caused by herpes simplex virus (HSV-1 or HSV-2), miscellaneous bacteria, or Acanthamoeba (especially in contact lens wearers).
HSV-1 keratitis is the leading infectious cause of blindness in the U.S.

Treatment: Trifluridine, acyclovir, or both; rigorous contact lens hygiene is essential to prevent Acanthamoeba keratitis.
