 Back
BackMedically Important Gram-Positive Bacilli: Structure, Pathogenesis, and Clinical Relevance
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Medically Important Gram-Positive Bacilli
Overview of Gram-Positive Bacilli
Gram-positive bacilli are a diverse group of bacteria that include both endospore-forming and non-endospore-forming genera. Many are significant human pathogens, causing a range of diseases from mild food poisoning to life-threatening systemic infections.
Endospore-formers: Bacillus, Clostridium, Clostridiodes
Non-endospore-formers: Listeria, Erysipelothrix, Actinomyces, Nocardia, Corynebacterium
Bacillus Species
General Characteristics of Bacillus
Bacillus species are Gram-positive, endospore-forming, motile rods commonly found in soil. They are obligate aerobes or facultative anaerobes and are catalase positive. Many species are saprobes and are a source of antibiotics. Of nearly 250 species, Bacillus anthracis and Bacillus cereus are clinically significant.
Endospore formation: Central endospores develop under all conditions except in the living body.
Motility: Most species are motile.
Antibiotic production: Some species are sources of medically important antibiotics.

Bacillus anthracis and Anthrax
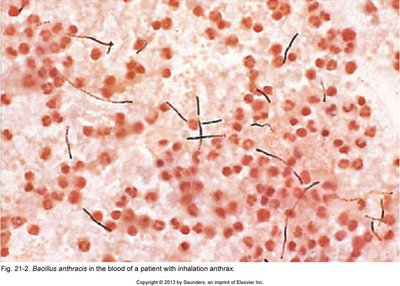
Bacillus anthracis is the causative agent of anthrax, a zoonotic disease with three clinical forms: cutaneous, pulmonary, and gastrointestinal. The bacterium is characterized by large, block-shaped rods and central endospores.
Virulence factors: Capsule and three exotoxins (protective antigen, edema factor, lethal factor).
Protective antigen (PA): Entry pore for other toxins; target for vaccines.
Edema factor (EF): Increases cAMP, causing edema.
Lethal factor (LF): Protease that disrupts cell signaling, leading to cell death.
Clinical forms:
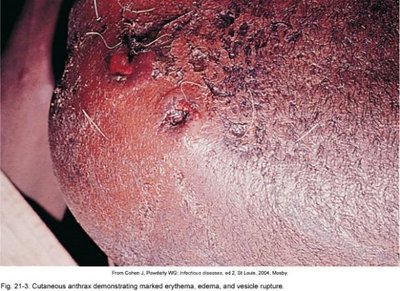
Cutaneous anthrax: Spores enter through skin, causing a black eschar. Least dangerous form.
Pulmonary anthrax: Inhalation of spores leads to severe respiratory distress and high mortality.
Gastrointestinal anthrax: Ingestion of spores; can cause severe systemic illness.

Diagnosis, Treatment, and Prevention
Diagnosis: Phage testing or direct fluorescent antibody (DFA) assays.
Treatment: Combination antibiotics (doxycycline with ciprofloxacin or penicillin; resistance possible).
Prevention: Decontamination of animal carcasses, sterilization of materials, and vaccination (purified toxoid for high-risk groups).
Bacillus cereus
Bacillus cereus is a common environmental bacterium that can cause foodborne illness. It produces both heat-stable and heat-labile enterotoxins.
Heat-stable enterotoxin: Causes emetic (vomiting) syndrome; rapid onset (1–6 hours), short duration (<24 hours).
Heat-labile enterotoxin: Causes diarrheal syndrome; may last longer.
Other infections: Can cause severe pneumonia, wound infections, and rapid-onset eye infections, especially in immunosuppressed individuals.
Treatment: Usually self-limited; severe cases may require antibiotics.

Clostridium and Clostridiodes
General Characteristics
Members of the genera Clostridium and Clostridiodes are Gram-positive, endospore-forming rods that are obligate anaerobes. They produce spores only under anaerobic conditions and are known for synthesizing organic acids, alcohols, and potent exotoxins.
Diseases: Cause wound infections, tissue infections, and food intoxications.
Clostridial Wound and Tissue Infections
Gas Gangrene (Clostridial Myonecrosis)
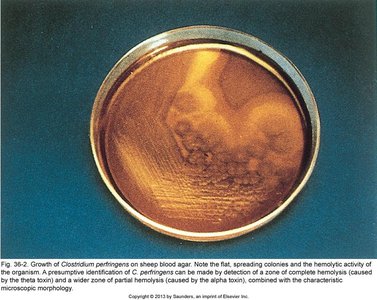
Gas gangrene is a severe infection caused primarily by Clostridium perfringens, but also by C. novyi and C. septicum. It is characterized by rapid tissue destruction, gas production, and high mortality if untreated.
Pathogenesis: Damaged tissue and anaerobic conditions allow spore germination, vegetative growth, and toxin release. Fermentation of muscle carbohydrates produces gas and further tissue destruction.
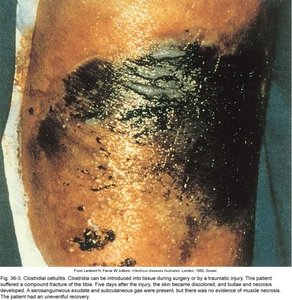
Predisposing factors: Surgical wounds, compound fractures, diabetic ulcers, septic abortions, deep wounds.
Clinical forms:
Anaerobic cellulitis: Localized infection of damaged tissue.
Myonecrosis: Toxins cause widespread muscle necrosis.


Treatment and Prevention of Gas Gangrene
Immediate cleansing and debridement of diseased tissue (including maggot therapy in some cases).
Protein synthesis inhibitors (e.g., clindamycin) to inhibit toxin production.
Hyperbaric oxygen therapy to increase tissue oxygenation and inhibit anaerobic growth.
Tetanus (Clostridium tetani)
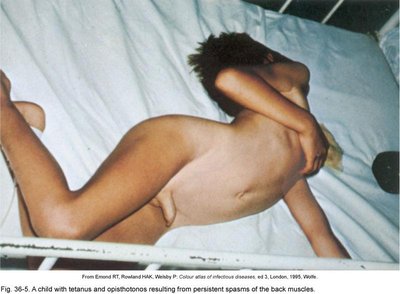
Clostridium tetani is a common soil and animal GI tract resident. It causes tetanus (lockjaw), a neuromuscular disease characterized by muscle rigidity and spasms.
Pathogenesis: Spores enter through wounds or umbilical stumps, germinate in anaerobic conditions, and release tetanospasmin (a neurotoxin).
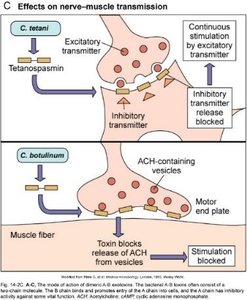
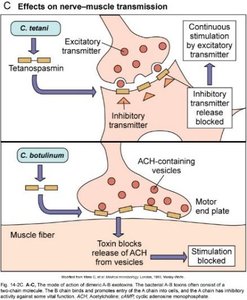
Tetanospasmin: Blocks inhibitory neurotransmitter release, causing uncontrolled muscle contraction and paralysis. Death is often due to respiratory muscle paralysis.
Prevention and Treatment of Tetanus
Wound cleaning and administration of antitoxin (TIG) to neutralize circulating toxin.
Antibiotics: Metronidazole is preferred; muscle relaxants may be used.
Prevention: Tetanus toxoid vaccine with boosters every 10 years.
Clostridial Food Poisoning
C. botulinum: Causes rare but severe botulism, usually from improperly canned foods. The botulinum toxin blocks acetylcholine release, leading to flaccid paralysis.
C. perfringens: Causes mild, self-limited gastroenteritis; common worldwide.
Botulism
Symptoms: Double/blurred vision, difficulty swallowing, flaccid paralysis.
Infant botulism: Ingestion of spores (e.g., in honey) leads to toxin production in the gut.
Wound botulism: Spores germinate in wounds and release toxin.
Clostridial Gastroenteritis
Agent: C. perfringens
Pathogenesis: Spores germinate in improperly cooked/stored food; exotoxin causes abdominal cramps and diarrhea.
Diagnosis: High numbers of Gram-positive rods in food or feces.
Clostridiodes difficile-Associated Disease (CDAD)
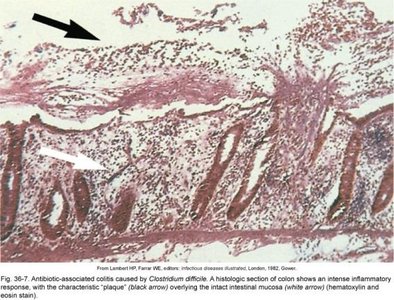
Clostridiodes difficile is a normal colon resident that can cause antibiotic-associated colitis when competing flora are suppressed. It produces enterotoxins that damage the intestinal lining, leading to severe diarrhea, especially in hospital settings.
Diagnosis: ELISA for toxins in stool.
Treatment: Supportive care, cessation of causative antibiotics, oral vancomycin or metronidazole, and fecal microbiota transplantation for severe cases.
Prevention: Strict infection control measures in healthcare settings.
Listeria monocytogenes
Characteristics and Pathogenesis
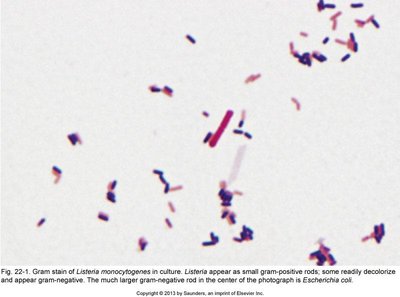
Listeria monocytogenes is a Gram-positive rod that can appear as coccobacilli or long filaments. It is motile, lacks a capsule, and is highly resistant to environmental stresses. It is a facultative intracellular pathogen, using listeriolysin O and ActA to survive and move within host cells.
Reservoirs: Soil, water, animal intestines; contaminates dairy, poultry, and meat products.
Growth: Can multiply at refrigeration temperatures.
Clinical significance: Causes listeriosis, which is mild in healthy adults but severe in pregnant women, neonates, elderly, and immunocompromised individuals (can cause meningitis and sepsis).
Diagnosis and Control
Diagnosis: Cold enrichment culture, ELISA, immunofluorescence, PCR.
Treatment: Ampicillin with trimethoprim/sulfamethoxazole.
Prevention: Pasteurization, thorough cooking, and use of bacteriophages in food safety.
Erysipelothrix rhusiopathiae
Characteristics and Clinical Significance
Erysipelothrix rhusiopathiae is a slender, easily decolorized, microaerophilic rod. It is a zoonotic pathogen, primarily affecting individuals who handle animals or fish.
Disease: Erysipeloid – a localized skin infection with fever and joint pain; rarely causes septicemia.

Filamentous Gram-Positive Bacilli
Actinomyces and Nocardia
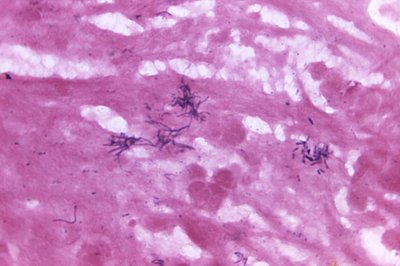
These genera are nonmotile, filamentous bacteria. Actinomyces species are part of normal flora and are opportunistic pathogens, while Nocardia species are soil organisms, partially acid-fast, and aerobic.
Actinomyces: Associated with dental plaque, caries, and chronic infections of skin and soft tissues (actinomycosis).
Nocardia: Causes pulmonary infections resembling tuberculosis, brain abscesses, and mycetoma (chronic, destructive infection of tissue and bone).
Diagnosis: Size and morphology are important; fungi may appear similar on Gram stain but are larger.

Corynebacterium diphtheriae
Characteristics and Pathogenesis
Corynebacterium diphtheriae is an irregularly staining, club-shaped, catalase-positive Gram-positive rod. It is carried by healthy individuals and transmitted via respiratory droplets. Most cases occur in non-immunized individuals in crowded, unsanitary conditions.
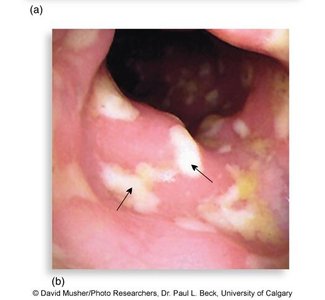
Pathogenesis: Two stages – local infection of the upper respiratory tract (sore throat, pseudomembrane formation, risk of asphyxiation) and systemic diphtherotoxin toxemia (affecting heart and nerves, 5–10% mortality).
Diphtherotoxin: Encoded by a bacteriophage; inhibits protein synthesis by inactivating elongation factor 2 (EF-2).
Alternative presentation: Cutaneous ulcers (can be caused by C. diphtheriae or C. ulcerans).
Diagnosis, Treatment, and Prevention
Diagnosis: Gray pseudomembrane, stains, serology, Elek test for antitoxin binding.
Treatment: Antitoxin (from CDC), penicillin or erythromycin.
Prevention: Diphtheria toxoid vaccine series and boosters.
