Back
BackMicrobiology of Skin and Eye Infections: Structure, Defenses, and Pathogens
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Overview of Skin Structure and Defenses
Skin Anatomy and Protective Mechanisms
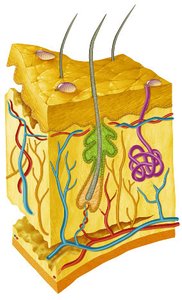
The skin is the largest organ of the human body and serves as a primary barrier against microbial invasion. Its structure and secretions provide both physical and chemical defenses.
Epidermis: Outermost layer, composed of tightly packed epithelial cells, provides a physical barrier.
Dermis: Contains connective tissue, blood vessels, nerves, hair follicles, and glands.
Subcutaneous Layer: Fatty tissue that insulates and cushions the body.
Defensive Secretions:
Melanin: Pigment that offers UV protection.
Perspiration (Sweat): Acidic pH and high salt content inhibit microbial growth; contains lysozyme which breaks down bacterial cell walls.
Sebum: Oily, acidic substance from sebaceous glands that inhibits some pathogens.
Normal Skin Microbiota
The skin hosts a diverse microbiome, with different microbes predominating in oily, moist, or dry regions. These normal residents help prevent colonization by pathogens.
Common Bacterial Phyla: Actinobacteria, Bacteroidetes, Proteobacteria.
Common Genera: Staphylococcus, Pseudomonas, Janthinobacterium, Malassezia (fungus).
Locations: Epidermis, sweat glands, sebaceous glands, hair follicles.
Factors Influencing Microbiota: Skin type (oily, moist, dry), hygiene, environment, and host genetics.
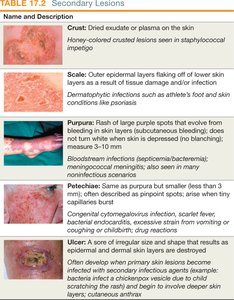
Clinical Terminology of Skin Lesions and Rashes
Understanding lesion terminology is essential for diagnosis and communication in clinical microbiology.
Lesion: Any change or abnormality in the skin, localized or widespread.
Primary Lesion: Directly associated with a disease process (e.g., vesicle, macule, papule, pustule, cyst).
Secondary Lesion: Develops from a primary lesion or as a result of external factors (e.g., crust, scale, ulcer).
Rash: Widespread eruption of lesions, may be symptomatic or asymptomatic.

Viral Skin Infections
Chickenpox and Shingles
Chickenpox and shingles are caused by the varicella-zoster virus (VZV), a member of the Herpesviridae family. The virus is highly contagious and can establish latency in nerve cells.
Transmission: Respiratory droplets and direct contact with lesions.
Pathogenesis: Virus enters via the respiratory tract, spreads through the blood, and causes skin lesions. It can become latent in peripheral nerves and reactivate as shingles.
Prevention: Chickenpox vaccine (since 1995) and shingles vaccine (Zostavax®) for older adults.

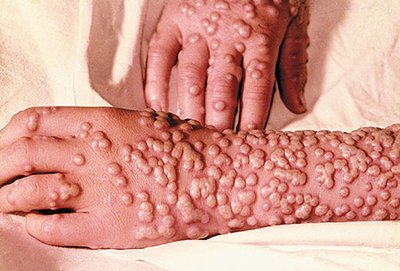
Smallpox
Smallpox, caused by the variola major virus (Poxviridae), was a highly contagious and deadly disease eradicated by vaccination.
Transmission: Respiratory droplets or contact with contaminated fomites.
Symptoms: High fever, fatigue, followed by pustular rash.
Mortality: Up to 30%.
Eradication: WHO vaccination program ended natural cases by 1980.
Herpes Simplex Virus 1 (HSV-1)
HSV-1 causes oral herpes, characterized by cold sores. The virus can establish latency in nerves and reactivate, causing recurrent lesions.
Transmission: Saliva, contaminated fomites.
Symptoms: Painful, itchy vesicular lesions on lips, sore throat, flu-like symptoms.
Latency: Virus remains dormant in nerves and can reactivate.
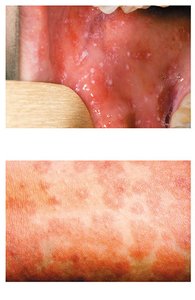
Measles (Rubeola)
Measles is a highly contagious viral disease with significant complications, preventable by the MMR vaccine.
Transmission: Respiratory droplets.
Symptoms: Fever, sore throat, dry cough, Koplik's spots in the mouth, maculopapular rash starting on the face and spreading.
Complications: Hospitalization, brain swelling, death.
Prevention: MMR vaccine (live attenuated).
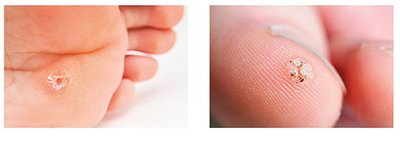
Warts (Papillomavirus)
Warts are benign skin growths caused by human papillomaviruses (HPV). They are generally harmless and self-limiting.
Transmission: Direct or indirect contact through skin abrasions.
Treatment: Cryotherapy, cauterization, laser removal, chemicals.
Bacterial Skin Infections
Acne (Propionibacterium acnes)
Acne is a common skin condition caused by the proliferation of Propionibacterium acnes in clogged pores, leading to inflammation.
Mechanism: Sebum and dead skin cells block pores, allowing bacterial growth and inflammation.
Treatment: Retinoids, antibiotics, benzoyl peroxide, photodynamic and laser therapies.
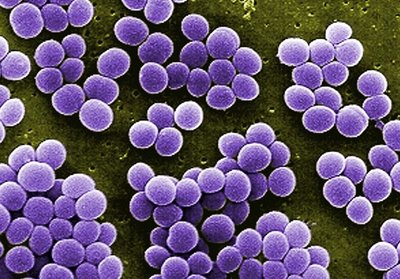
Staphylococcus aureus Infections
Staphylococcus aureus is a Gram-positive coccus that forms clusters and produces numerous virulence factors, causing a range of skin diseases.
Virulence Factors: Coagulase, catalase, hemolysins, M-protein.
Diseases: Impetigo, cellulitis, abscesses.
Laboratory Characteristics: Catalase positive, mannitol fermenter, beta-hemolytic, coagulase positive.
Staphylococcal Impetigo
Highly contagious, especially in children.
Symptoms: Superficial pus-filled vesicles, honey-colored crusted lesions.
Treatment: Topical antibiotics.

Cellulitis
Infection of lower dermis and subcutaneous fat.
Symptoms: Red, swollen, painful skin, fever, may spread to lymph nodes and bloodstream.
Treatment: Antibiotics; MRSA complicates treatment.

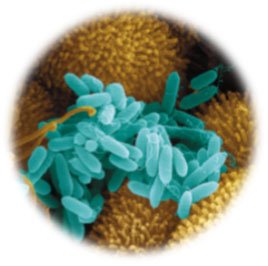
Pseudomonas Infections
Pseudomonas aeruginosa is a Gram-negative rod, opportunistic pathogen, and common cause of healthcare-associated infections (HAIs).
Virulence: Forms biofilms, produces pigments (e.g., pyocyanin), highly antibiotic-resistant.
Diseases: Wound infections, otitis externa (swimmer's ear).
Treatment: Meticulous wound care, antibiotics, silver creams, debridement.

Otitis Externa (Swimmer's Ear)
Infection of the outer ear canal, often due to P. aeruginosa.
Risk Factors: Poorly maintained pools, hot tubs.
Treatment: Antibiotic eardrops.

Gas Gangrene (Clostridium perfringens)
Gas gangrene is a severe infection of deep wounds by Clostridium perfringens, an anaerobic, endospore-forming bacterium.
Symptoms: Foul-smelling gas, tissue destruction, shock, kidney failure.
Treatment: Antibiotics, debridement, amputation, hyperbaric oxygen.

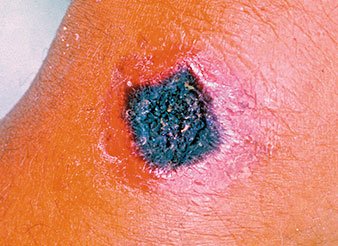
Cutaneous Anthrax (Bacillus anthracis)
Cutaneous anthrax is caused by Bacillus anthracis, a Gram-positive, endospore-forming bacterium.
Transmission: Entry through skin wounds, contact with infected animals or products.
Symptoms: Solid nodule, blackened ulcer (eschar), painless but may itch.
Treatment: Antibiotics.
Fungal Skin Infections
Cutaneous Mycoses
Fungal infections of the skin are usually superficial and caused by Candida species or dermatophytes.
Dermatophytes: Infect skin, hair, and nails, causing brittleness and flaking.
Treatment: Removal of affected hair, topical or oral antifungals.
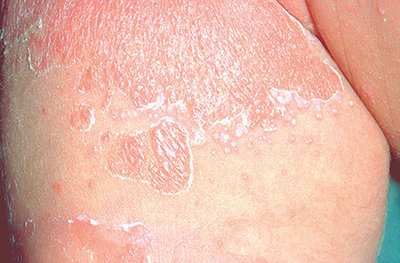
Cutaneous Candidiasis
Agent: Candida albicans, a unicellular yeast.
Symptoms: Bright red macular rash, white pustules, itching/burning, scaling.
Treatment: Keep area dry, topical creams.

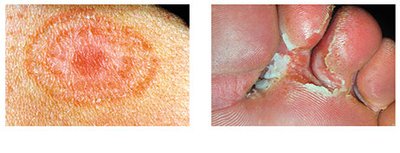
Tinea Infections (Ringworm)
Transmission: Skin abrasions, fomites, contact with infected people or animals.
Symptoms: Scaly, blistered, discolored, or inflamed skin; hair discoloration or bald patches.
Treatment: OTC topical antifungals, prescription oral drugs.
Parasitic Skin Infections
Leishmaniasis
Leishmaniasis is caused by protozoan Leishmania species, transmitted by sand fly bites. It is prevalent in tropical and subtropical regions.
Cutaneous Leishmaniasis: Painless ulcers at bite sites, can persist for months or years, may scar.
Mucocutaneous Leishmaniasis: Lesions in mucous membranes, severe disfigurement.
Visceral Leishmaniasis: Systemic spread, fatal if untreated.
Prevention: Avoid sand fly bites (protective clothing, repellents).
Treatment: Chemotherapy (species-dependent).

Structure, Defenses, and Infections of the Eyes
Eye Structure and Defense Mechanisms
The eye is protected by multiple anatomical and chemical barriers that limit microbial colonization.
Cornea: Multiple layers of epithelial cells at the front of the eye.
Conjunctiva: Mucous membrane covering the eyeball and lining the eyelids.
Lacrimal Gland: Produces tears containing lysozyme (breaks down bacterial cell walls) and lactoferrin (binds iron).
Normal Eye Microbiota
The ocular surface is colonized by a limited but distinct microbiome, with different species dominating the conjunctiva and cornea.
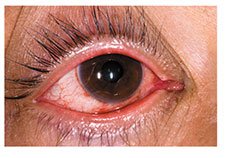
Viral Conjunctivitis
Viral conjunctivitis is most commonly caused by adenoviruses and is highly contagious.
Symptoms: Red or pink, swollen conjunctiva; itchy, painful, watery eyes; usually starts in one eye.
Transmission: Direct contact, fomites, vertical transmission (HSV in neonates).
Prevention: Hand hygiene, avoid sharing personal items.
Treatment: Usually self-limiting; avoid contact lenses during infection.
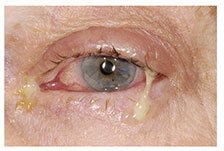
Bacterial Conjunctivitis
Bacterial conjunctivitis is caused by various bacteria, including Haemophilus influenzae, Staphylococcus, and Streptococcus species.
Symptoms: Similar to viral conjunctivitis, but with pus-like discharge (often green or yellow), eyelids may be crusted.
Treatment: Often mild and self-resolving; antibiotic eye drops or ointment may be used.
Neonatal Bacterial Conjunctivitis
Causes: Neisseria gonorrhoeae or Chlamydia trachomatis, acquired during birth.
Prevention: Antibiotic drops for all newborns in the U.S.

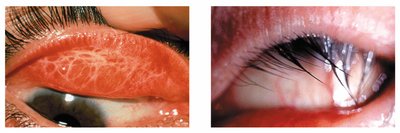
Trachoma
Trachoma is a chronic conjunctivitis caused by certain types of Chlamydia trachomatis. It is the leading infectious cause of blindness worldwide.
Symptoms: Rough conjunctiva, scarring, inward-turning eyelids, corneal damage.
Transmission: Contaminated fomites, hands, or flies.
Prevention: Facial hygiene, environmental improvements.
Treatment: Oral azithromycin, ophthalmic ointments, surgery for eyelid correction.
Keratitis
Keratitis is inflammation of the cornea, caused by viruses, bacteria, protozoa, or helminths.
Viral Keratitis: Most commonly due to HSV-1; symptoms include conjunctivitis, eye pain, blurred vision, sensitivity to light.
Bacterial Keratitis: Often caused by Pseudomonas aeruginosa or Staphylococcus aureus; associated with improper contact lens use.
Protozoan Keratitis: Acanthamoeba species; linked to poor contact lens hygiene.
Helminthic Keratitis (River Blindness): Onchocerca volvulus larvae migrate to the eye, causing inflammation and blindness.
Treatment: Antivirals (trifluridine, acyclovir), antibiotics, antiparasitics (ivermectin, doxycycline).