 Back
BackAssessment of the Heart and Neck Vessels: Clinical and Developmental Perspectives
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
The Heart and Neck Vessels
Overview
The assessment of the heart and neck vessels is a fundamental component of personal health and clinical practice. This process involves gathering a detailed health history, performing a systematic physical examination, and understanding developmental variations across the lifespan. Mastery of these skills is essential for identifying cardiovascular health and disease.

Health History
Key Components of Cardiovascular Health History
Chest Pain: Assess for the presence, character, and duration of chest pain. The clenched fist sign is a classic indicator.
Dyspnea: Shortness of breath, including dyspnea on exertion (DOE), paroxysmal nocturnal dyspnea (PND), and orthopnea (difficulty breathing when lying flat).
Cough: Persistent cough may indicate heart failure or pulmonary congestion.
Fatigue: Unusual tiredness, especially with exertion, can be a sign of decreased cardiac output.
Edema: Swelling of the lower extremities may suggest heart failure.
Cyanosis/Pallor: Bluish or pale skin may indicate poor perfusion or oxygenation.
Nocturia: Frequent urination at night, often associated with heart failure.
Past and Family Cardiac History: Includes previous heart disease, surgeries, and family history of cardiovascular conditions.
Personal Habits: Smoking, diet, exercise, and alcohol use are important risk factors.
Developmental Considerations in Health History
Infants: Focus on maternal health, feeding patterns, growth, and activity levels.
Children: Assess growth, activity (e.g., squatting, knee-chest position), joint pain, fever, headaches, nosebleeds, and frequent respiratory infections.
Pregnant Individuals: Monitor for hypertension, faintness, and dizziness.
Older Adults: Evaluate for heart/lung disease, medication use, and environmental factors. Be aware of increased risk factors with age.



Physical Assessment Preparation
Preparation and Positioning
Carotid Arteries: Patient should be sitting up for assessment.
Precordium & Jugular Veins: Patient should be supine with the head elevated to 30 degrees.
Abnormal Heart Sounds: Best heard with the patient in the left lateral position.
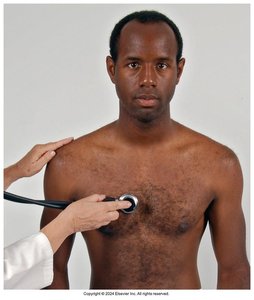
Examiner Position: Stand on the patient's right side and explain the necessity of multiple auscultation points.
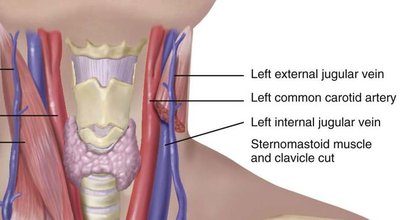
Neck Vessels
Carotid Arteries
The carotid arteries supply blood to the brain and are assessed for patency and abnormal sounds.
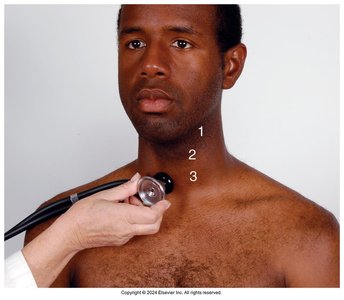
Auscultation: Performed with the neck in a neutral position, using the bell of the stethoscope to detect bruits. The patient should hold their breath briefly. Auscultate before palpating, in three areas: angle of jaw, mid-cervical, and base of neck.
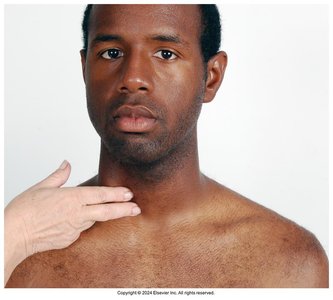
Palpation: Palpate medial to the sternomastoid muscle, avoiding excessive pressure on the carotid sinus. Palpate one artery at a time and note the strength.
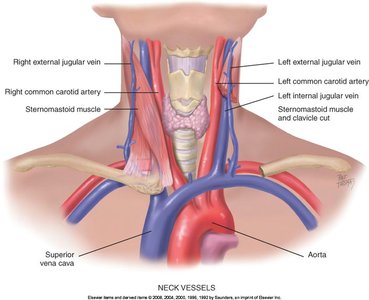
Jugular Veins
Jugular veins provide information about central venous pressure (CVP) and right heart function.
Inspection: The external jugular vein is more visible, but the internal jugular vein is a more reliable indicator of CVP. The head should be elevated 30-45 degrees, and tangential lighting is used to observe pulsations.
Clinical Note: The internal jugular vein cannot be seen directly; its pulsations are observed indirectly.
Precordium Assessment
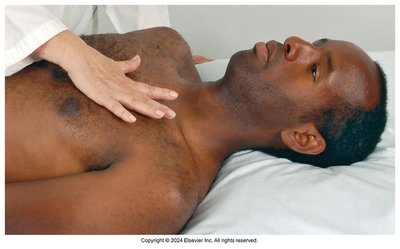
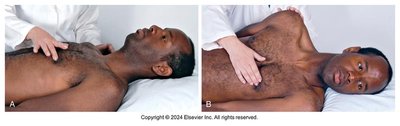
Inspection and Palpation
Apical Impulse: Inspect and palpate for the apical impulse, typically visible at the 4th or 5th intercostal space (ICS) at the midclavicular line (MCL). Note location, size, amplitude, and duration. It may not be palpable in obese individuals or those with thick chest walls.
Palpation Across Precordium: Palpate the apex, left sternal border, and base for abnormal pulsations or thrills (vibratory sensations).
Percussion
Limited Usefulness: Percussion is rarely used but may help assess cardiac enlargement by percussing from the left 5th ICS anterior axillary line (AAL) to the 2nd ICS across to the sternal border.
Auscultation
Auscultation is the primary method for evaluating heart sounds and function.
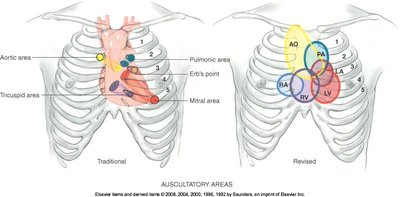
Valve Areas: Four main areas are auscultated:
Aortic: 2nd ICS at right sternal border
Pulmonic: 2nd ICS at left sternal border
Tricuspid: 4th/5th ICS at left sternal border
Mitral: 5th ICS at left MCL
Sequence: Use a Z-pattern across the precordium, with the patient in different positions. Begin with the diaphragm, then use the bell for low-pitched sounds.
Assess: Rate and rhythm, S1/S2, extra sounds, and murmurs.
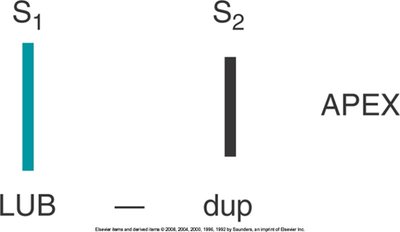
Heart Sounds
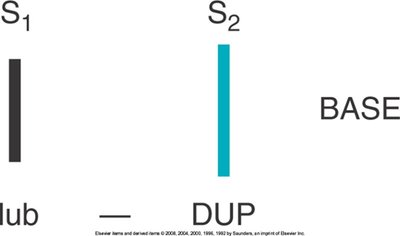
S1 ("lub"): Closure of atrioventricular (A-V) valves, marks the beginning of systole, louder at the apex. Coincides with the carotid pulse and the R wave on ECG.
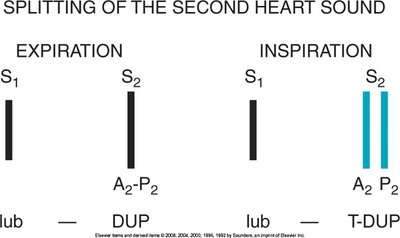
S2 ("dup"): Closure of semilunar valves, marks the end of systole, louder at the base.
Splitting: Split S1 is rare but normal in the tricuspid area; split S2 is normal at the end of inspiration in the pulmonic area.
Extra Heart Sounds and Murmurs
Extra Sounds: S3 and S4 may be normal or abnormal. S3 is associated with rapid ventricular filling; S4 with atrial contraction.
Murmurs: Blowing or swooshing sounds due to turbulent blood flow. Assessed for timing, loudness (graded I-VI), pitch, quality, pattern, location, radiation, and changes with posture.
Types: Innocent murmurs (no pathology), functional murmurs (increased blood flow), and pathological murmurs (structural heart disease).
Grade | Description |
|---|---|
I | Barely audible |
II | Audible but faint |
III | Moderately loud, easy to hear |
IV | Loud, palpable thrill |
V | Very loud, heard with stethoscope partly off chest |
VI | Loudest, heard with stethoscope just off chest |
Developmental Considerations
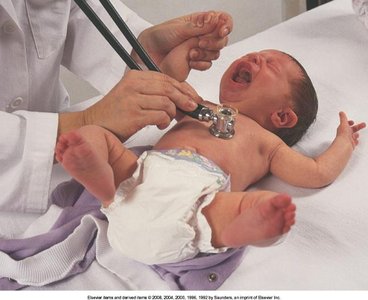
Infants
Fetal Shunts: Close within 10-15 hours after birth; assess in the first 24 hours and again at 2-3 days.
Apical Impulse: Located at the 4th ICS lateral to MCL.
Sinus Arrhythmia: Common with respiratory cycle.
Murmurs: Common in the first 2-3 days of life.
Children
Apical Impulse: Varies with age: 4th ICS left of MCL (<4 years), 4th ICS MCL (4-6 years), 5th ICS right of MCL (7 years).
Venous Hum: Common and usually benign.
Innocent Murmurs: Present in up to 30% of children.
Pregnant Individuals
Resting Pulse: Increases by 10-15 beats per minute.
Blood Pressure: Decreases in the second trimester, increases in the third.
Heart Displacement: Upward and to the left due to uterine enlargement.
Systolic Murmur: Present in up to 90% of pregnancies.
Mammary Souffle: Murmur heard near term or during lactation.
Older Adults
Systolic Blood Pressure: Gradually increases with age.
Carotid Assessment: Requires caution due to increased risk of atherosclerosis.
S4: Common in older adults due to decreased ventricular compliance.
Premature Ectopic Beats: Common and often benign.
Orthostatic Hypotension: Increased risk due to impaired autonomic response.
Additional info: Understanding the normal and abnormal findings in heart and neck vessel assessment is crucial for early detection of cardiovascular disease and for tailoring care to specific populations, including infants, children, pregnant individuals, and older adults.
