 Back
BackDeath and Dying: Chapter 59
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Death and Dying
Introduction
End-of-life care is a critical aspect of health care, especially for Certified Nursing Assistants (CNAs) who support dying patients in various settings. While most people express a desire to die at home, the majority pass away in hospitals or nursing homes. Understanding the needs of dying individuals and their families is essential for providing compassionate and effective care.
End of life care: Support provided during the time nearing death, focusing on comfort and dignity.
Terminal illness: An illness with no expectation of recovery.
Hospice care: Care for those expected to die within six months, emphasizing physical, emotional, social, and spiritual needs rather than cure.
Palliative care: Focuses on symptom relief and may include treatment of the illness.
Attitudes About Death
Influences on Attitudes
Attitudes toward death are shaped by personal experiences, culture, religion, and age. Some individuals fear death, while others accept it. Adults often worry about pain, suffering, dying alone, and the impact on loved ones.
Culture and religion: Influence beliefs about the afterlife and the body after death.
Reincarnation: The belief that the spirit or soul is reborn in another form.
Stages of Dying (Elisabeth Kübler-Ross)
The Five Stages
Elisabeth Kübler-Ross identified five stages that people may experience when facing death. Not everyone goes through all stages or in a specific order.
Denial: Refusal to accept impending death.
Anger: Feelings of resentment or envy toward others.
Bargaining: Attempting to negotiate for more time, often with a higher power.
Depression: Mourning for losses and the future.
Acceptance: Achieving peace and calmness about death.
Psychological, Social, and Spiritual Needs
Supporting the Dying Person
Dying individuals may need to talk, express emotions, or seek spiritual support. Listening and presence are vital, even if the person does not wish to speak. Respect for their wishes and spiritual needs is essential.
Offer to listen or simply sit with them.
Facilitate visits from spiritual leaders if desired.
Show courtesy and respect at all times.
Physical Needs at End of Life
General Physical Changes
The dying process can be rapid or gradual. Maintaining dignity and comfort is crucial. Common physical changes include blurred vision, impaired speech, and hearing loss (often the last sense to diminish). Nutrition may become difficult, so offer small, frequent meals as tolerated.
Oral Care
Oral hygiene is important for comfort, especially if the person cannot eat or drink. Provide oral care at least every two hours if the patient is not taking fluids.
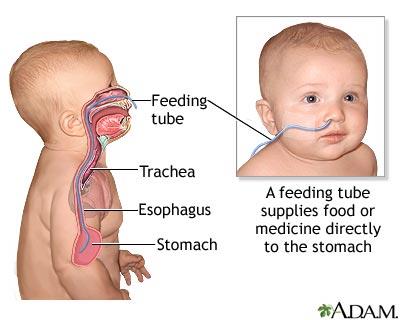
Nasal Care
Nasal secretions, oxygen tubing, and nasogastric (NG) tubes can cause crusting and irritation. Clean the nose gently and apply lubricant as directed by the nurse.
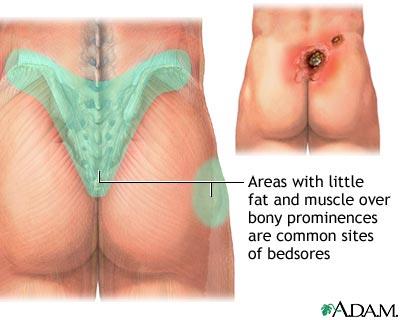
Skin Care
Decreased circulation can cause the skin to feel cool, pale, and mottled. Frequent repositioning and gentle back massages help maintain comfort and prevent pressure ulcers (bedsores).
Elimination
Urinary incontinence and retention are common. Provide frequent perineal care and use catheters if necessary. Constipation may require enemas.
Pain Management
Fear of pain is common among dying patients. Pain medications are usually available, but families may have concerns about hastening death, addiction, or clouding consciousness. Address these concerns with sensitivity and provide comfort-focused care.
Family Support
Involving and Supporting Families
Families may wish to stay with the dying person and participate in care. They may experience a range of emotions, including sadness, anger, and grief. Be courteous, considerate, and supportive.
Do’s and Don’ts of Helping the Grieving Family
Do: Listen more than you talk, allow silence, answer questions, be genuine, and let them express feelings without judgment.
Don’t: Dominate conversation, ask too many questions, use clichés, pass judgment, avoid them, change the subject, or feel you must have all the answers.
Legal Concerns
Patient Rights and Advance Directives
Patients have the right to refuse life-sustaining treatments and make advance directives. These legal documents state a person's wishes about health care when they cannot make decisions themselves.
Living will: Specifies measures to support or maintain life when death is likely.
Durable power of attorney for health care: Appoints another person to make health care decisions (Health Care Proxy).
“Do Not Resuscitate” (DNR) Orders
DNR orders allow patients to die with dignity, without resuscitation attempts. Comfort measures continue, regardless of DNR status. Health care providers must respect these orders, even if they personally disagree.
Quality of Life
Patient Rights in Nursing Centers
Patients have the right to privacy, confidentiality, freedom from abuse, personal possessions, and a safe, home-like environment. Personal choice and dignity must be respected before and after death.
Signs of Approaching Death
Physical and Behavioral Signs
Restlessness, agitation, or withdrawal
Drowsiness, increased sleep, or unresponsiveness
Confusion or disorientation
Changes in breathing patterns
Decreased need for food and fluids
Loss of bowel or bladder control
Skin coolness and mottling
Increased pain
Signs of Death
No breathing or pulse
Pupils dilated, eyes do not blink
Jaw relaxed, mouth open
Release of bowel and bladder contents
No response to stimuli
Care of the Body After Death
Postmortem Care
Postmortem care involves cleaning and positioning the body, respecting privacy and dignity. Rigor mortis sets in within 2–4 hours. Tubes and catheters are removed only as directed. Personal belongings are gathered for the family, and identification tags are applied according to policy.
Close the eyes and mouth (use a rolled towel under the chin if needed).
Insert dentures or place them in a labeled cup.
Remove jewelry except wedding rings (tape in place).
Brush hair and dress in a clean gown.
After family viewing, cover the body with a sheet or shroud and attach ID tags.
Conclusion
Dying is more than a medical event; it is a unique, personal experience. Health care providers should approach end-of-life care with empathy, attention, and respect, ensuring dignity for both the dying person and their family.
