 Back
BackThe Ear: Structure, Function, and Health Assessment
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
The Ear: Anatomy and Health Assessment
Overview of Ear Structure and Function
The ear is a complex organ responsible for hearing and balance. It is divided into three main sections: the external ear, middle ear, and inner ear. Each section plays a critical role in the process of sound transmission and equilibrium.
External Ear: Includes the auricle (pinna) and external auditory canal, which collect and direct sound waves toward the tympanic membrane.
Middle Ear: Contains the tympanic membrane and ossicles (malleus, incus, stapes) that transmit vibrations to the inner ear.
Inner Ear: Houses the cochlea for hearing and the vestibular apparatus for balance.

External Ear: Anatomy and Inspection
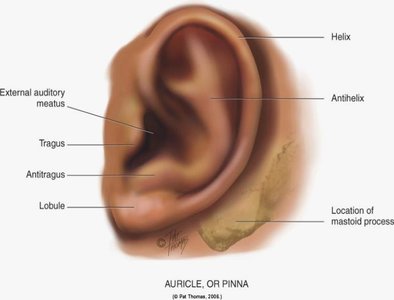
The external ear consists of the auricle (pinna) and the external auditory meatus. Inspection and palpation (I & P) of the external ear are essential in clinical assessment to identify abnormalities in size, shape, position, and skin condition.
Auricle (Pinna): The visible part of the ear, composed of cartilage and skin, helps funnel sound into the ear canal.
Landmarks: Helix, antihelix, tragus, antitragus, lobule, and mastoid process.
Normal Variants: Darwin’s tubercle is a small, painless nodule at the helix, considered a normal anatomical variant.
Assessment of Ear Alignment
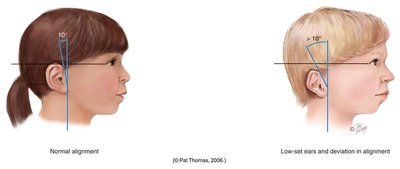
Proper alignment of the ears is important, especially in pediatric assessment. Low-set or abnormally aligned ears may indicate congenital anomalies or syndromes.
Normal Alignment: The top of the auricle should align with the outer canthus of the eye and be angled no more than 10 degrees from the vertical plane.
Abnormal Alignment: Low-set or deviated ears may be associated with genetic conditions.
Health History: Key Questions
Taking a thorough health history is essential for identifying ear problems. Important questions include:
Presence of earache or pain
History of infections or discharge
Hearing loss or changes in hearing
Exposure to environmental noise
Symptoms such as tinnitus (ringing) or vertigo (dizziness)
Self-care practices (e.g., ear cleaning methods)
Special Considerations for Infants and Children: Ask about frequent ear infections, hearing milestones, and any history of trauma or injury.
Physical Examination: Preparation and Techniques
Proper preparation and technique are crucial for an accurate ear examination. The examiner should ensure the patient is comfortable and explain the procedure to reduce anxiety, especially in children.
Inspect and palpate the external ear for tenderness, discharge, or abnormalities.
Examine the external auditory meatus for cerumen (earwax) or signs of infection.

Otoscope Examination
An otoscope is used to visualize the ear canal and tympanic membrane. Proper technique varies by age:
Speculum Selection: Choose the largest speculum that fits comfortably in the ear canal.
Positioning: For adults, pull the pinna up and back; for children under 3 years, pull the pinna straight down.
Timing: Perform the otoscopic exam before hearing tests to avoid altering the ear canal environment.


Normal Tympanic Membrane
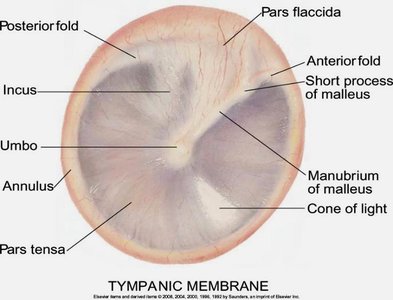
The tympanic membrane (eardrum) should appear pearly gray, translucent, and intact. Key features include:
Cone of Light Reflex: A reflection of light seen in the anteroinferior quadrant, indicating a healthy membrane.
Mobility: The membrane should move with pressure changes.
Intactness and Scarring: Look for perforations or evidence of previous infections.
Common Ear Pathologies
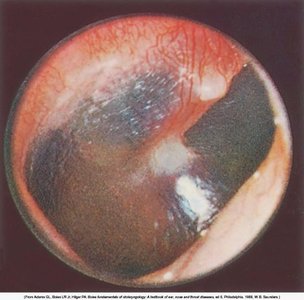
Otitis media (middle ear infection) and ruptured tympanic membrane are common findings, especially in children.
Otitis Media: Inflammation and infection of the middle ear, often presenting with a red, bulging tympanic membrane.
Ruptured Membrane: Perforation may result in discharge and hearing loss.

Hearing Acuity and Vestibular Function
Screening for hearing deficits is an important part of the ear exam. Simple bedside tests include the whispered voice test. The vestibular apparatus is assessed using the Romberg test for balance.
Whispered Voice Test: Assesses gross hearing ability but does not quantify hearing loss.
Romberg Test: Evaluates balance; a normal result is the ability to stand with minimal swaying for 20 seconds.

Developmental Considerations
Ear anatomy and examination techniques vary by age. Special approaches are needed for infants, children, and older adults.
Infants and Children
Position of Pinna: Pull straight down for children under 3 years during otoscopic exam.
Exam Technique: Stabilize the child's head, use games or demonstrations to reduce fear, and perform the exam on the parent's lap if needed.
Newborns: May have an "injected" (reddened) tympanic membrane.
Children: Ear canal is more horizontal; pneumatic otoscopy may be used to assess membrane mobility.
T-tubes: Small tubes inserted to ventilate the middle ear in children with recurrent infections.
Developmental Milestones: Monitor for behavioral signs of hearing loss, such as delayed speech or inattentiveness.



Aging Adults
Pendulous Earlobes: Earlobes may become elongated and wrinkled with age.
Tympanic Membrane: May appear whiter and more opaque.
Impacted Cerumen: Earwax buildup is common and can cause hearing loss.
Presbycusis: Age-related sensorineural hearing loss, typically affecting high-frequency sounds first.

Transcultural Considerations
Otitis media is the most common illness in children worldwide. Cerumen (earwax) type is genetically determined and varies among populations.
Otitis Media: Higher prevalence in certain ethnic groups and environments.
Cerumen Type: Can be wet or dry, with genetic factors influencing its characteristics.
