 Back
BackThe Respiratory System: Assessment and Anatomy for Personal Health
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
The Respiratory System
Overview
The respiratory system is essential for gas exchange, supplying oxygen to the body and removing carbon dioxide. Understanding its structure and function is crucial for personal health and clinical assessment.
Major components: Nose, pharynx, larynx, trachea, bronchi, lungs
Main function: Facilitate the exchange of gases between the air and blood
Clinical relevance: Assessment of respiratory health is vital for detecting diseases and maintaining overall wellness

Thoracic Anatomy and Landmarks
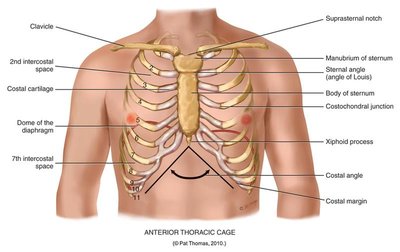
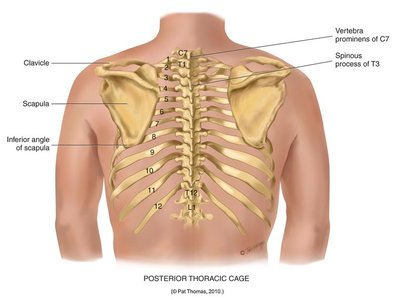
Thoracic Cage and Landmarks
The thoracic cage protects the lungs and heart, and provides attachment points for respiratory muscles. Accurate identification of anatomical landmarks is essential for physical examination.
Anterior landmarks: Clavicle, suprasternal notch, sternal angle, costal cartilage, xiphoid process, costal margin
Posterior landmarks: Vertebra prominens (C7), scapula, spinous processes, inferior angle of scapula
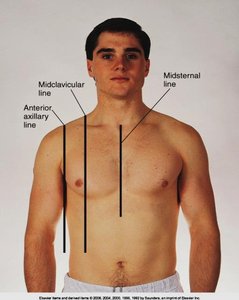
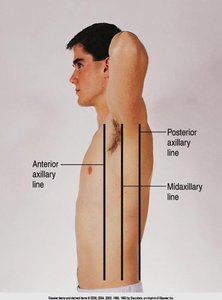
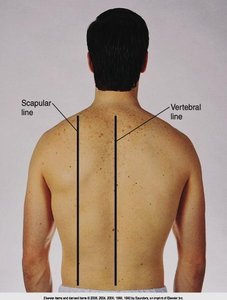
Reference Lines
Reference lines are used to describe locations on the thorax for assessment and documentation.
Anterior: Midsternal, midclavicular, anterior axillary lines
Lateral: Anterior, midaxillary, posterior axillary lines
Posterior: Vertebral, scapular lines
Lung Anatomy
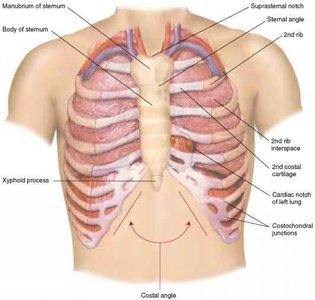
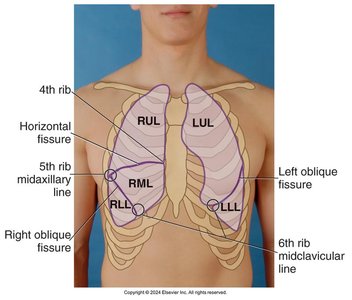
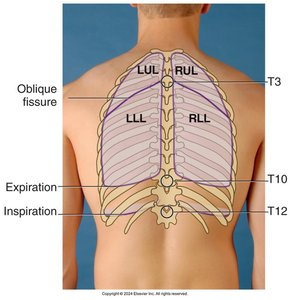
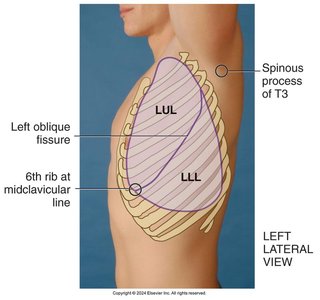
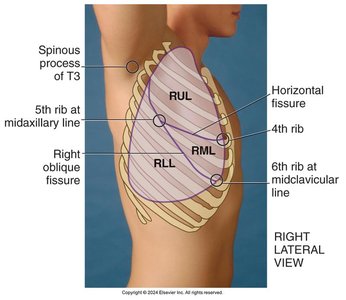
Lobes of the Lungs
The lungs are divided into lobes, each with distinct anatomical boundaries. Understanding lobe locations is important for targeted assessment and diagnosis.
Right lung: Three lobes (upper, middle, lower)
Left lung: Two lobes (upper, lower)
Fissures: Horizontal and oblique fissures separate the lobes
Health History and Physical Examination
Health History
Collecting a thorough health history is the first step in respiratory assessment. Key areas include:
History of respiratory illnesses (asthma, COPD, pneumonia, etc.)
Smoking history and exposure to environmental hazards
Family history of respiratory diseases
Current symptoms: cough, shortness of breath, chest pain, sputum production
Physical Examination Techniques
Physical examination of the respiratory system involves inspection, palpation, percussion, and auscultation.
Inspection: Observe chest shape, symmetry, and respiratory effort
Palpation: Assess for symmetrical chest expansion and tactile fremitus
Percussion: Evaluate underlying tissue density (resonance, dullness)
Auscultation: Listen for breath sounds and identify abnormalities
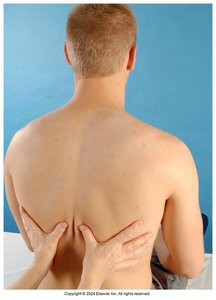
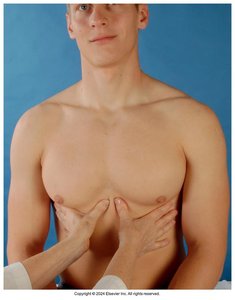
Tactile Fremitus
Tactile fremitus is the palpable vibration transmitted through the bronchopulmonary tree to the chest wall when a patient speaks.
Assessed using the ulnar edge or ball of the hand
Patient repeats phrases like "99" or "blue moon"
Decreased fremitus may indicate obstruction; increased fremitus may indicate consolidation
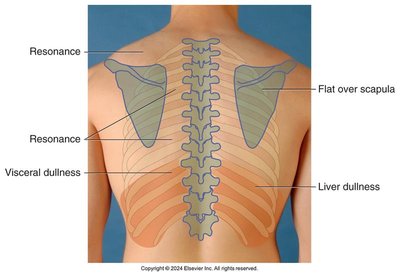
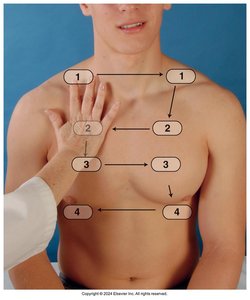
Percussion and Auscultation
Percussion
Percussion helps determine the underlying tissue's density and can identify areas of abnormality.
Normal percussion note over healthy lung tissue is resonance
Dullness may indicate consolidation, tumor, or organ (e.g., liver)
Tympany may be heard over the stomach

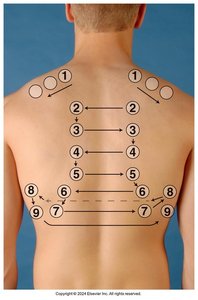
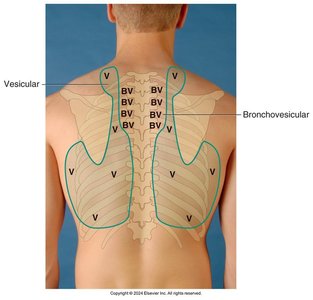
Auscultation
Auscultation is used to assess the quality and type of breath sounds in different lung fields.
Three main types of breath sounds: Bronchial, Bronchovesicular, and Vesicular
Normal locations for each type should be noted
Abnormal sounds (crackles, wheezes, rhonchi) may indicate pathology

Pulmonary Function Measurements
Key Measurements
Pulmonary function tests (PFTs) assess lung capacity and airflow, providing important information about respiratory health.
Tidal Volume (TV): Volume of air inhaled or exhaled in a normal breath
Vital Capacity (VC): Maximum amount of air exhaled after a maximum inhalation
Forced Expiratory Volume (FEV1): Volume of air exhaled in the first second of a forced breath
Formula for Vital Capacity:
Where:
VC: Vital Capacity
TV: Tidal Volume
IRV: Inspiratory Reserve Volume
ERV: Expiratory Reserve Volume
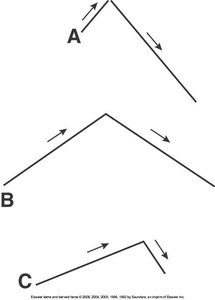
Developmental Considerations
Infants and Children
Respiratory assessment in infants and children requires special considerations due to anatomical and physiological differences.
Infants have a rounder chest (AP:Transverse ratio 1:1)
By age 6, the chest ratio approaches adult proportions (1:2)
Breath sounds may be louder and more bronchovesicular in peripheral fields in children under 6
Apgar Scoring System
The Apgar score is used to quickly assess the health of newborns immediately after birth. It evaluates five criteria: heart rate, respiratory effort, muscle tone, reflex irritability, and color.
Characteristic | Score 2 | Score 1 | Score 0 |
|---|---|---|---|
Heart rate | Over 100 | Slow (below 100) | Absent |
Respiratory Effort | Good, sustained cry; regular respiration | Slow, irregular, shallow | Absent |
Muscle tone | Active motion, spontaneous flexion | Some flexion of extremities, some resistance to extension | Limp, flaccid |
Reflex Irritability | Sneeze, cough, cry | Grimace, frown | No response |
Colour | Completely pink | Body pink, extremities pale | Cyanotic, pale |
Summary
Understanding the anatomy and assessment of the respiratory system is fundamental for personal health and clinical practice. Accurate history taking, physical examination, and knowledge of normal and abnormal findings are essential for early detection and management of respiratory conditions.
