 Back
BackPsychological Disorders: History, Diagnosis, and the Justice System
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Psychological Disorders and Mental Health
Defining Mental Illness
Mental illness is defined by the DSM as patterns of behavior or experience that cause distress, impair day-to-day functioning, or increase the risk of harm. However, this definition is not perfect, as some maladaptive behaviors may not be classified as mental illnesses, and some individuals may be considered mentally ill without clearly meeting these criteria.
Maladaptive Behavior: Actions that interfere with daily life or pose risks.
Distress: Emotional suffering is a key component.
Impairment: Difficulty functioning in social, occupational, or other important areas.
Historical Conceptions of Mental Illness
Views on mental illness have evolved significantly over time, from supernatural explanations to medical models.
Demonic Model: In the Middle Ages, odd behaviors were attributed to evil spirits, leading to exorcisms and witch hunts.
Medical Model: During the Renaissance, mental illness was seen as a physical disorder requiring treatment, often in asylums with practices like bloodletting and snake pits.
Moral Treatment: Reformers such as Phillippe Pinel and Dorothea Dix advocated for humane treatment, allowing patients more freedom and dignity, though effective treatments were still lacking.



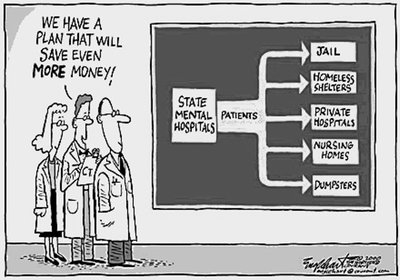
Modern Era and Deinstitutionalization
The development of antipsychotic medications like chlorpromazine (Thorazine) in the 1950s led to deinstitutionalization, releasing patients from hospitals but often without adequate community support.
Chlorpromazine: Reduced symptoms of schizophrenia and similar disorders.
Deinstitutionalization: Shifted care from hospitals to community settings, sometimes resulting in homelessness or incarceration.

Diagnosis and Classification
DSM-5 and the Biopsychosocial Model
The DSM-5 is the official classification system for mental disorders, providing diagnostic criteria and decision rules. It emphasizes ruling out medical or substance-related causes and adopts a biopsychosocial approach.
Biological Factors: Brain chemistry, genetics, neurodevelopment, physical health.
Psychological Factors: Cognitive patterns, emotional regulation, personality, coping skills.
Social Factors: Environment, culture, family dynamics, socioeconomic status.
Explosion of Diagnoses
The number of diagnoses in the DSM has increased dramatically, raising concerns about over-treatment and the influence of the insurance industry.
DSM Version | Year | No. Diagnoses |
|---|---|---|
DSM I | 1952 | 106 |
DSM II | 1968 | 182 |
DSM III | 1980 | 265 |
DSM IV | 1994 | 365 |
DSM 5 | 2013 | 400+ |
Culture and Mental Disorders
Culture-Bound Syndromes
Certain mental disorders are influenced by cultural context, while others (e.g., schizophrenia, alcoholism, psychopathy) are universal.
Malocchio: Italian syndrome involving headaches, fatigue, anxiety, and bad luck caused by envy.
Calor do corpo/nervos: Portuguese syndrome involving fatigue, anxiety, and gastrointestinal issues attributed to bodily imbalance.
Taijin Kyofusho: Japanese social anxiety characterized by fear of offending others, reflecting collectivist cultural values.


Major Psychological Disorders
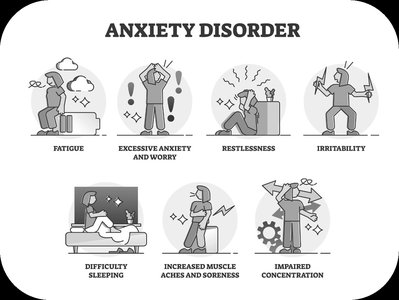
Anxiety-Related Disorders
Anxiety disorders are characterized by distressing, persistent anxiety or maladaptive behaviors that reduce anxiety. They include generalized anxiety disorder, panic disorder, specific phobias, OCD, and PTSD.
Generalized Anxiety Disorder: Continual feelings of worry, tension, and irritability about many areas.
Panic Disorder: Repeated, unexpected panic attacks and persistent concern about future attacks.
Phobias: Unrealistic fear of specific situations, activities, or objects.
Obsessive-Compulsive Disorder: Intrusive thoughts (obsessions) and ritualistic behaviors (compulsions).
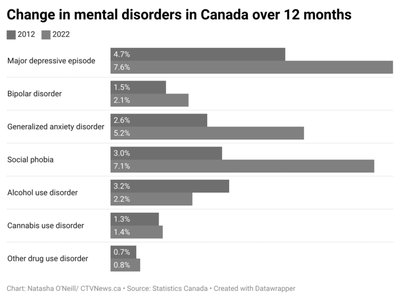
Mood Disorders
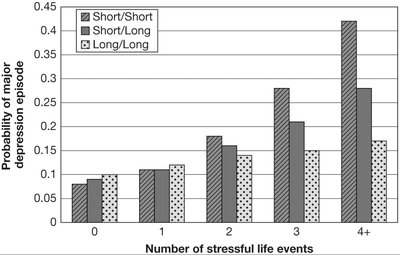
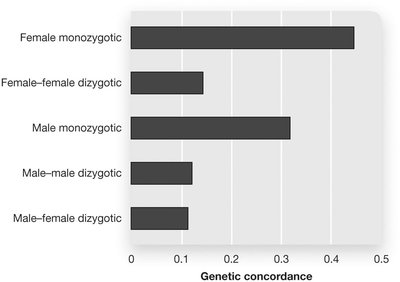
Mood disorders include depression and bipolar disorder, affecting nearly 10% of adults in Canada and the US. Depression is more common among women and those living in poverty, with genetic and environmental risk factors.
Major Depression: Periods of sadness, hopelessness, social withdrawal, and cognitive/physical sluggishness.
Bipolar Disorder: Extreme shifts in mood, motivation, and energy, with periods of depression and mania.



Schizophrenia
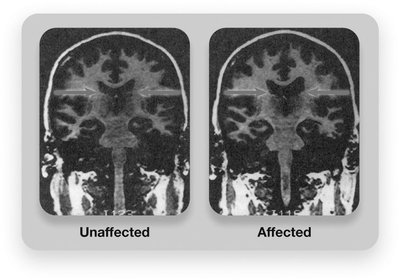
Schizophrenia involves significant breaks from reality, lack of integration of thoughts and emotions, and problems with attention and memory. Symptoms are classified as positive (hallucinations, delusions) and negative (absence of adaptive behavior).
Brain Structure: Larger ventricles, loss of brain tissue, differences in hippocampus and amygdala.
Brain Activity: Reduced activity in frontal lobes and emotion/memory regions.
Neurotransmitters: Dopamine overactivity linked to positive symptoms; glutamate underactivity may play a role.
Environmental Causes: Extreme stress, low SES, minority status, prenatal environment, cannabis use.

Personality Disorders
Personality disorders are characterized by unusual patterns of behavior that are maladaptive, distressing, and resistant to change. They are grouped into three clusters:
Cluster A: Odd or eccentric behavior (e.g., paranoid, schizoid).
Cluster B: Dramatic, emotional, erratic behavior (e.g., antisocial, narcissistic).
Cluster C: Anxious, fearful, inhibited behavior (e.g., avoidant).
Borderline Personality Disorder
Borderline personality disorder involves intense emotional swings, unstable sense of self, impulsivity, and difficult social relationships. It is often rooted in emotional insecurity and early adverse experiences.
Antisocial Personality Disorder and Psychopathy
Antisocial personality disorder (APD) is marked by a profound lack of empathy, disregard for others' rights, and violent tendencies. Psychopathy is an extreme form of APD with additional interpersonal and emotional traits.
Factor 1: Interpersonal/emotional (glibness, grandiosity, lack of remorse).
Factor 2: Social deviance (impulsivity, need for stimulation).
Brain Differences: Under-reactive to stress, amygdala abnormalities, frontal lobe impairments.
Uncommon Psychiatric Syndromes
Capgras's Syndrome: Belief that a loved one has been replaced by a double.
Ekbom's Syndrome: Delusions of infestation.
Munchausen Syndrome: Fabrication of medical symptoms leading to unnecessary treatment.
Mental Illness and the Justice System
Insanity Defense and NCRMD
The insanity defense (NCRMD: Not Criminally Responsible by Reason of Mental Disorder) is a legal concept, not a psychological one. Criminal guilt requires both actus reus (the guilty action) and mens rea (the guilty mind). Mental illness can negate mens rea.
Current Test (Canadian Criminal Code S. 16): No person is criminally responsible if, at the time of the offense, they were suffering from a mental disorder that rendered them incapable of appreciating the nature and quality of the act or knowing it was wrong.
Possible Outcomes: Absolute discharge, conditional discharge, or detention in a hospital, decided by a Review Board.

Myths and Realities of NCRMD
Myth: Frequently used; Reality: Used in only 1% of felony cases, fails 75% of the time.
Myth: Loophole for the guilty; Reality: Most NCR defendants spend their sentence in jail or hospital.
Myth: Extremely dangerous; Reality: Most NCR cases are non-violent.
Myth: Quick release; Reality: NCR individuals are committed longer than if found guilty.
Mental Health in the Correctional System
Mental illness is significantly more common in prison than in the general population. Incarceration often worsens mental health due to harsh conditions, lack of services, and overuse of segregation.
Prevalence: ~70% of federally incarcerated individuals report mental health symptoms.
Segregation: 22% of inmates placed in segregation; 42%+ of segregated inmates had a mental health alert.
Effects: Hallucinations, cognitive disabilities, insomnia, self-harm, paranoia, suicidal tendencies.
Case Studies
Kalief Browder: Held in solitary for 700+ days, never recovered from trauma.
Edward Snowshoe: Spent 162 days in solitary, died by suicide.
Ashley Smith: Four years in isolation, committed suicide.
Community Support and Advocacy
Organizations such as the John Howard Society, Fred Victor, Elizabeth Fry Society, AMHO, CMHA, and CAMH work to support individuals with mental illness and reduce conflict with the law.
Summary Table: Major Psychological Disorders
Disorder | Key Features | Treatment |
|---|---|---|
Anxiety Disorders | Persistent anxiety, maladaptive behaviors | Therapy, medication |
Mood Disorders | Depression, bipolar disorder | Therapy, medication |
Schizophrenia | Breaks from reality, hallucinations, delusions | Antipsychotics, therapy |
Personality Disorders | Maladaptive, distressing, resistant to change | Therapy, sometimes medication |
