 Back
BackTreatment of Psychological Disorders: Modern Approaches and Effectiveness
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Treatment of Psychological Disorders
Historical and Social Context
The treatment of psychological disorders has evolved significantly from the 1400s to the present. Early institutions were often inhumane, and treatments were largely ineffective. The discovery of antipsychotic medications in the 1960s led to deinstitutionalization, shifting care to community settings. However, this shift has contributed to increased rates of homelessness and justice involvement among individuals with mental illness.
Deinstitutionalization: Movement from long-term psychiatric hospitals to community-based care.
Current challenges: High rates of mental health issues among homeless populations, youth, and Indigenous peoples in Canada.
Legal involvement: Courts may mandate treatment through community treatment orders for individuals exhibiting severe symptoms.
Example: Ontario has considered policies for forced treatment in crisis situations, sparking debate over individual rights versus public safety.
Access to Mental Health Services
Modern mental health care is delivered through a variety of sources, each with specific roles and limitations.
Psychiatric hospitals: Short-term care for acute crises; involuntary admission possible if risk of harm is present.
Primary care: Family doctors provide initial assessment and referrals.
Psychiatrists: Medical doctors who can prescribe medication.
Psychologists and therapists: Provide talk therapy and assessments, but cannot prescribe medication.
Community services: Offer low-cost support, crisis intervention, and case management.
Barriers to treatment: Stigma, cultural attitudes, gender roles, financial and geographical obstacles.
Cultural and Gender Barriers
Cultural background and gender norms significantly influence attitudes toward mental health treatment.
Cultural barriers: Lower rates of help-seeking among Asian Canadians and Indigenous peoples; therapy is more accepted in individualistic cultures.
Masculinity norms: Men may avoid treatment due to beliefs about self-reliance and stigma around emotional disclosure.
Types of Psychological Therapies
Insight Therapies
Insight therapies focus on increasing self-awareness and understanding of psychological conflicts through dialogue.
Psychoanalysis: Developed by Freud; aims to uncover unconscious conflicts using techniques like free association and dream analysis.
Resistance: Client's reluctance to discuss certain topics, interpreted by the therapist.
Transference: Redirecting feelings for significant others onto the therapist.
Psychodynamic therapy: Modern, shorter-term version focusing on early relationships and emotional attachments.
Evaluation: Some empirical support, especially for panic disorder and borderline personality disorder.
Person-Centered Therapy
This humanistic approach emphasizes the therapeutic relationship, empathy, and unconditional positive regard to foster self-actualization and healing.
Non-directive: The therapist provides support without directing the client's choices.
Therapeutic alliance: A strong relationship predicts better outcomes.
Behavioral Therapies
Behavioral therapies apply principles of learning to modify maladaptive behaviors.
Classical conditioning techniques:
Aversive conditioning: Pairing unwanted behavior with unpleasant stimuli (e.g., Antabuse for alcohol use).
Systematic desensitization: Gradual exposure to feared stimuli while practicing relaxation techniques.
Flooding: Rapid, intense exposure to feared stimuli to extinguish anxiety.
Operant conditioning techniques:
Token economies: Rewarding desirable behaviors with tokens.
Contingency contracting: Written agreements outlining behavioral goals and consequences.
Observational learning: Modeling adaptive behaviors (e.g., "Fearless Peer").
Advantages: Effective for phobias, compulsions, and skill-building. Disadvantages: Limited insight into underlying thoughts; less effective for severe depression.
Cognitive-Behavioural Therapies (CBT)
CBT combines cognitive and behavioral techniques to address dysfunctional thinking and behavior. It is the most widely used therapy today.
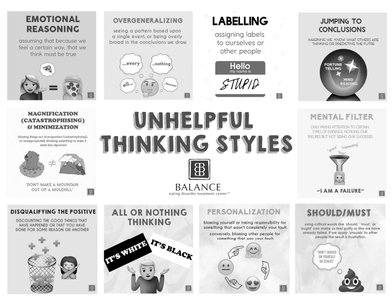
Cognitive restructuring: Identifying and challenging negative thought patterns.
Exposure: Facing avoided situations to reduce anxiety.
Relaxation: Techniques to regain emotional control.
Homework: Practice and application outside of sessions.
Dysfunctional thinking patterns in depression: Internal, stable, and global attributions (e.g., "It's all my fault," "It will never change," "My whole life is ruined").
Example: CBT is effective for anxiety, depression, substance abuse, and eating disorders.
Dialectical Behavioural Therapy (DBT)
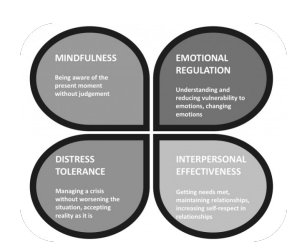
DBT is a form of CBT that emphasizes acceptance and change, particularly for individuals with personality disorders.
Distress tolerance: Managing crises without worsening the situation.
Mindfulness: Focusing on the present moment without judgment.
Emotional regulation: Understanding and managing emotions.
Interpersonal effectiveness: Maintaining relationships and self-respect.
Effectiveness: Promising results, especially for borderline personality disorder.
Other Cognitive-Behavioral Approaches
Interoceptive exposure therapy: Used for panic disorder; clients are exposed to physical sensations of panic in a controlled way to reduce fear.
Mindfulness-Based Cognitive Therapy (MBCT): Combines mindfulness meditation with CBT techniques to help clients "decenter" from their thoughts.
Group and Family Therapies
Group and family therapies provide support, advice, and skill-building in a collective setting. Types include self-help groups (e.g., Alcoholics Anonymous) and family therapy to improve communication and roles.
Advantages: Economical, peer support, tailored to group needs.
Disadvantages: May not always involve a professional therapist.
Effectiveness of Psychotherapy
Research shows that psychotherapy is effective for most people, though not universally. Different therapies are suited to different problems, and therapists often use an eclectic approach.
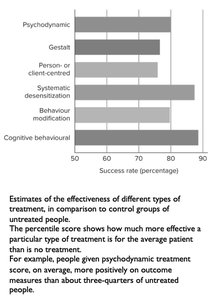
Example: Cognitive-behavioral and systematic desensitization therapies show the highest success rates.
Biomedical Therapies
Pharmacological Treatments
Antipsychotic drugs: Block dopamine receptors to reduce psychotic symptoms; newer drugs may increase dopamine in specific brain areas.
Antianxiety drugs: Benzodiazepines (e.g., Xanax, Valium) enhance GABA activity but carry risks of dependence and respiratory depression.
Antidepressants:
Tricyclics: Increase norepinephrine.
MAO inhibitors: Prevent breakdown of serotonin and other neurotransmitters.
SSRIs: Selectively increase serotonin at synapses (e.g., Prozac, Zoloft).
Herbal remedies: St. John's Wort may reduce depression but is unregulated and can interact with other medications.
New directions: Ketamine therapy for treatment-resistant depression; concerns about cognitive effects and addiction.
Non-Pharmacological Biomedical Treatments
Transcranial Magnetic Stimulation (TMS): Non-invasive magnetic pulses stimulate specific brain regions; effective for depression but may cause seizures.
Electroconvulsive Therapy (ECT): Electric currents induce seizures to treat severe depression; controversial due to potential memory loss and unknown mechanisms.
Psychosurgery: Rare, last-resort procedures for severe cases (e.g., OCD, depression); modern techniques are more precise than historical lobotomies.
Other Controversial Treatments
Eye Movement Desensitization and Reprocessing (EMDR): Involves recalling traumatic events while performing eye movements; evidence for effectiveness is limited and controversial.
Critical Perspectives
On Being Sane in Insane Places (Rosenhan, 1970s)
This classic study demonstrated the challenges of psychiatric diagnosis and the depersonalization experienced by patients in mental hospitals. Sane individuals feigned symptoms to gain admission and were subsequently treated as mentally ill, highlighting the need for critical evaluation of mental health systems.
