 Back
BackBlood: Structure, Function, and Clinical Significance
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Blood: Structure, Function, and Clinical Significance
Functions of Blood
Blood is a specialized connective tissue that serves as the internal transport system of the body. Its functions are categorized into transport, regulation, and protection.
Transport: Delivers oxygen (O2) and nutrients to cells, removes metabolic wastes, and transports hormones.
Regulation: Maintains body temperature, pH balance (via buffers and bicarbonate ions), and fluid volume in the circulatory system.
Protection: Prevents blood loss (clot formation) and infection (via antibodies, complement proteins, and white blood cells).
Components of Blood
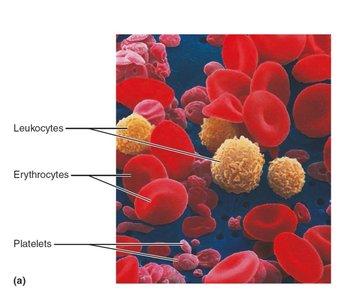
Blood consists of cellular elements (formed elements) suspended in plasma, a fluid matrix. The formed elements include erythrocytes (RBCs), leukocytes (WBCs), and platelets.
Erythrocytes: Red blood cells responsible for gas transport.
Leukocytes: White blood cells involved in immune defense.
Platelets: Cell fragments essential for clotting.
Physical Characteristics and Volume
Blood is a viscous, opaque fluid with a metallic taste. Its viscosity is about five times greater than water, primarily due to RBCs. The color varies with oxygen content: bright red when oxygen-rich, dark red when oxygen-poor. Blood pH ranges from 7.35 to 7.45, and it constitutes about 8% of body weight.
Average volume: 5–6 L in males, 4–5 L in females.
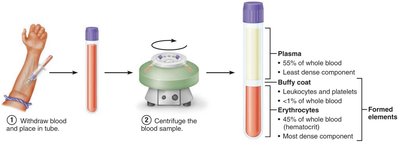
Blood Plasma
Plasma is the straw-colored, sticky fluid portion of blood, making up 55% of its volume. It is composed of:
Water: 90% of plasma volume; acts as a solvent and heat absorber.
Solutes: Over 100 dissolved substances, including nutrients, gases, hormones, wastes, proteins, and inorganic ions.
Plasma proteins: Most abundant solutes by weight (~8% of plasma), mainly produced by the liver. Key proteins include:
Albumin: ~60% of plasma proteins; regulates osmotic pressure and acts as a carrier and buffer.
Globulins: ~36%; includes transport proteins and antibodies.
Fibrinogen: ~4%; forms fibrin threads during clotting.
Formed Elements of Blood
The formed elements include erythrocytes, leukocytes, and platelets. Erythrocytes and platelets are not true cells (RBCs lack nuclei; platelets are fragments), while leukocytes are complete cells.
Erythrocytes (Red Blood Cells)
Structure and Function
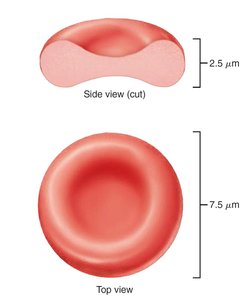
Erythrocytes are small, biconcave, anucleate cells optimized for gas exchange. Their shape increases surface area and shortens diffusion distance. They are filled with hemoglobin (Hb), which binds reversibly to oxygen and carbon dioxide.
Diameter: ~7.5 μm
Absence of mitochondria: Prevents consumption of transported oxygen; ATP is produced anaerobically.
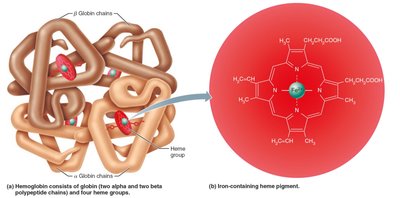
Hemoglobin Structure and Function
Hemoglobin is a protein composed of four globin chains (two alpha, two beta) and four heme groups, each with a central iron ion. Each iron binds one oxygen molecule, allowing each Hb to carry four oxygen molecules.
Oxygen loading: Forms oxyhemoglobin (bright red).
Oxygen unloading: Forms deoxyhemoglobin (dark red).
Carbon dioxide transport: 20% of CO2 binds to Hb, forming carbaminohemoglobin.
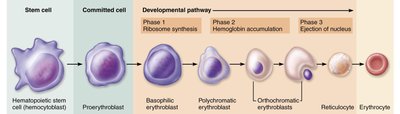
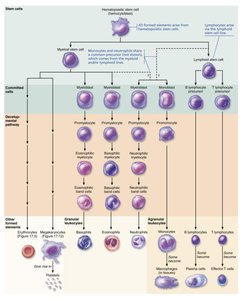
Erythropoiesis: Formation of Red Blood Cells
Erythropoiesis is the process of RBC production, occurring in red bone marrow. It involves several stages, starting from hematopoietic stem cells (hemocytoblasts) and progressing through committed progenitors to mature erythrocytes.
Reticulocytes: Immature RBCs; their count estimates RBC formation rate.
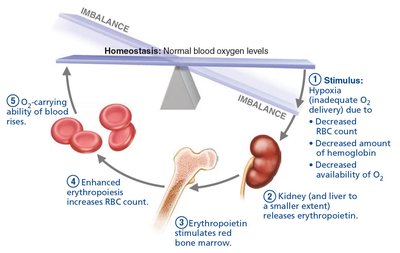
Regulation of Erythropoiesis
The number of circulating RBCs is tightly regulated by erythropoietin (EPO), a hormone produced by the kidneys in response to hypoxia (low oxygen levels). EPO stimulates RBC production in bone marrow.
Dietary requirements: Amino acids, lipids, carbohydrates, vitamin B12, folic acid, and iron.
Life Cycle and Destruction of Erythrocytes
RBCs have a lifespan of 100–120 days. Old RBCs are destroyed by macrophages in the spleen, liver, and bone marrow. Hemoglobin is broken down into heme (degraded to bilirubin), iron (stored for reuse), and globin (metabolized to amino acids).

Erythrocyte Disorders
Disorders include anemia (insufficient RBCs or hemoglobin) and polycythemia (excess RBCs).
Anemia: Causes include blood loss, insufficient RBC production, or excessive RBC destruction. Types include iron-deficiency, pernicious, renal, aplastic, hemolytic, thalassemia, and sickle-cell anemia.
Sickle-cell anemia: Caused by a mutation in the beta globin chain, resulting in crescent-shaped RBCs that rupture easily and block vessels.
Polycythemia: Abnormal excess of RBCs, increasing blood viscosity.

Leukocytes (White Blood Cells)
Structure and Function
Leukocytes are complete cells with nuclei and organelles, crucial for defense against disease. They move through tissues by diapedesis and chemotaxis.
Leukocytosis: Elevated WBC count, a normal response to infection.
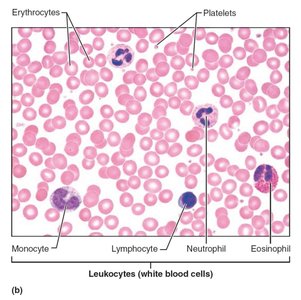
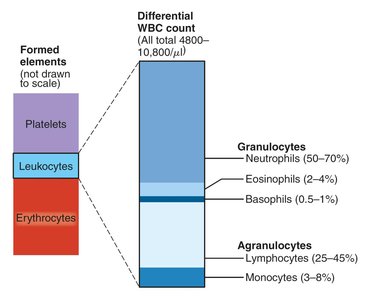
Classification: Granulocytes (neutrophils, eosinophils, basophils) and agranulocytes (lymphocytes, monocytes).
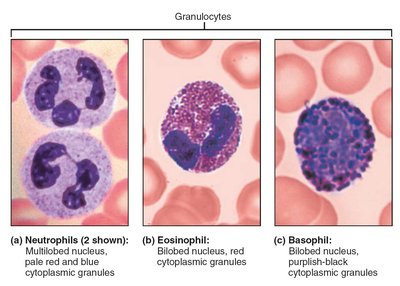
Granulocytes
Granulocytes have visible cytoplasmic granules and lobed nuclei. They include:
Neutrophils: Most numerous; phagocytize bacteria; granules contain defensins and enzymes.
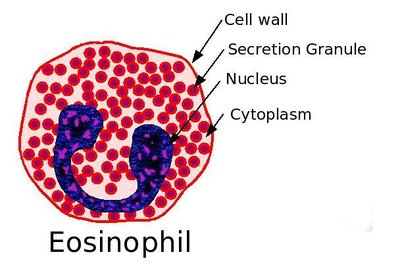
Eosinophils: Attack parasitic worms; modulate allergies and asthma.
Basophils: Rarest; release histamine and heparin, promoting inflammation.
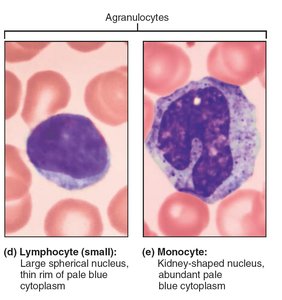
Agranulocytes
Agranulocytes lack visible granules and have spherical or kidney-shaped nuclei. They include:
Lymphocytes: Second most numerous; T cells attack infected cells and tumors, B cells produce antibodies.
Monocytes: Largest WBCs; differentiate into macrophages, active in phagocytosis and immune response.
Leukopoiesis: Formation of White Blood Cells
Leukopoiesis is stimulated by interleukins and colony-stimulating factors (CSFs). Hematopoietic stem cells differentiate into myeloid or lymphoid lines, producing various WBCs.
Leukocyte Disorders
Leukemia: Cancerous overproduction of abnormal WBCs; classified as acute or chronic, myeloid or lymphocytic.
Leukopenia: Abnormally low WBC count, often drug-induced.
Infectious mononucleosis: Viral disease (Epstein-Barr virus) causing excess atypical lymphocytes.
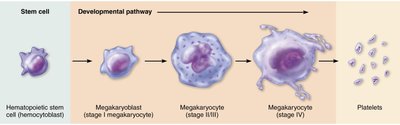
Platelets
Structure and Function
Platelets are fragments of megakaryocytes, containing granules with clotting chemicals. They form temporary plugs to seal vessel breaks and are regulated by thrombopoietin.
Normal concentration: 150,000–400,000 platelets/ml
Lifespan: 5–10 days
Summary Table: Formed Elements of Blood
Cell Type | Description | Count (cells/μL) | Development | Life Span | Function |
|---|---|---|---|---|---|
Erythrocytes | Biconcave, anucleate disc | 4–6 million | ~15 days | 100–120 days | Transport O2 and CO2 |
Neutrophils | Multilobed nucleus, granules | 3,000–7,000 | ~14 days | 6 hours–few days | Phagocytize bacteria |
Eosinophils | Bilobed nucleus, red granules | 100–400 | ~14 days | ~5 days | Kill parasitic worms, allergy/asthma |
Basophils | Bilobed nucleus, purplish-black granules | 20–50 | 1–7 days | Few hours–few days | Release histamine, contain heparin |
Lymphocytes | Spherical/indented nucleus, pale blue cytoplasm | 1,500–3,000 | Days–weeks | Hours–years | Immune response |
Monocytes | U/kidney-shaped nucleus, gray-blue cytoplasm | 100–700 | 2–3 days | Months | Phagocytosis, develop into macrophages |
Platelets | Discoid fragments, granules | 150,000–400,000 | 4–5 days | 5–10 days | Seal vessel tears, clotting |
Hemostasis: Prevention of Blood Loss
Steps of Hemostasis
Hemostasis is a rapid, localized process involving three steps:
Vascular spasm: Smooth muscle contracts, causing vasoconstriction.
Platelet plug formation: Platelets adhere to exposed collagen fibers and release chemicals to attract more platelets.
Coagulation: Fibrin proteins form a mesh that traps blood cells, forming a clot.

Disorders of Hemostasis
Thromboembolic disorders: Undesirable clot formation (thrombus, embolus).
Bleeding disorders: Platelet or clotting factor deficiencies (thrombocytopenia, hemophilia).
Disseminated intravascular coagulation (DIC): Both widespread clotting and severe bleeding.

Blood Transfusion and Blood Typing
Blood Groups and Compatibility
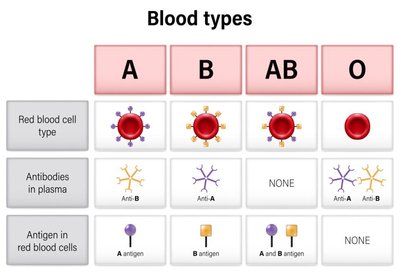
Blood groups are determined by antigens (agglutinogens) on RBC membranes. The ABO and Rh groups are most clinically significant.
ABO groups: Type A (A antigen), Type B (B antigen), Type AB (A and B antigens), Type O (no antigens).
Antibodies: Anti-A and/or anti-B antibodies present in plasma, depending on blood type.
Rh group: Rh+ (D antigen present), Rh− (D antigen absent).
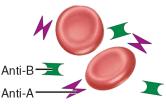
Blood Typing and Transfusion Reactions
Blood typing involves mixing blood with antibodies against common antigens. Agglutination indicates the presence of the antigen. Transfusion reactions occur if mismatched blood is infused, leading to agglutination and destruction of donor RBCs.

Clinical Significance of Blood Tests
Blood tests provide valuable information about a patient's health:
Hematocrit: Indicates anemia or polycythemia.
Blood glucose: Checks for diabetes.
Leukocyte count: Signals infection or immune disorders.
Prothrombin time and platelet count: Assess hemostasis.
Complete blood count (CBC): Evaluates formed elements, hematocrit, and hemoglobin.
Developmental Aspects of Blood
Fetal blood cells form in the yolk sac, liver, and spleen. Red bone marrow becomes the primary hematopoietic site by the seventh month. The fetus produces hemoglobin F, which has a higher affinity for oxygen than adult hemoglobin A.
Additional info: These notes expand upon the original lecture slides and textbook images, providing definitions, examples, and clinical context for each topic. All included images directly reinforce the adjacent explanations.
