 Back
BackMetabolism and Energy Balance: Regulation, Hormones, and Homeostasis
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Metabolism and Energy Balance
Metabolic Primer
Metabolism refers to the set of life-sustaining chemical transformations within the cells of living organisms. These transformations involve energy substrates—carbohydrates, fats, and proteins—which can be directed toward storage (anabolism) or breakdown (catabolism). The regulation of metabolism is primarily endocrine, with the insulin/glucagon ratio playing a central role, and is also influenced by neural mechanisms, especially in the regulation of food intake.
Anabolism: Synthesis and storage of biomolecules.
Catabolism: Breakdown of biomolecules for energy.
Key regulators: Insulin (promotes storage), Glucagon (promotes breakdown).
Fates of Ingested Biomolecules
After ingestion, biomolecules have three possible fates:
Fuel: Metabolized to provide energy.
Build: Used in synthesis reactions for growth and maintenance.
Store: Stored as glycogen (in liver and skeletal muscle) or fat (in adipose tissue).
Metabolism is divided into two states:
Fed (absorptive) state: Anabolic, products of digestion are absorbed and used for synthesis or storage.
Fasted (postabsorptive) state: Catabolic, body taps into stored reserves.
Regulation of Metabolism: Insulin and Glucagon
Enzymes control the direction of metabolism, and their activity is regulated by hormones. In the fed state, insulin promotes anabolic processes, while in the fasted state, glucagon stimulates catabolic pathways.
Insulin: Increases activity of enzymes for glycogen synthesis, inhibits enzymes for glycogen breakdown.
Glucagon: Activates enzymes for glycogen breakdown, inhibits glycogen synthesis.
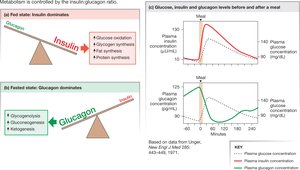
Fed vs. Fasted State
Fed State: Insulin dominates, promoting glucose oxidation, glycogen synthesis, fat synthesis, and protein synthesis.
Fasted State: Glucagon dominates, promoting glycogenolysis, gluconeogenesis, and ketogenesis.
Interconversions of Carbohydrate, Fat, and Protein
Metabolic pathways allow for the conversion between carbohydrates, fats, and proteins. Key processes include glycolysis, gluconeogenesis, lipolysis, and ketogenesis.
Glycogenolysis: Breakdown of glycogen to glucose.
Gluconeogenesis: Synthesis of glucose from non-carbohydrate sources.
Ketogenesis: Formation of ketone bodies from fatty acids during prolonged fasting or low carbohydrate intake.
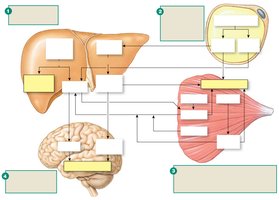
Nutrient Storage Depots
During the fasted state, the body relies on stored nutrients:
Carbohydrates: Glycogen in liver (exportable as glucose) and muscle (used locally or exported as lactate/pyruvate).
Fats: Triglycerides in adipose tissue (exported as fatty acids and glycerol).
Proteins: Muscle proteins broken down to amino acids for gluconeogenesis.
Ketogenesis and Ketoacidosis
When lipolysis exceeds the capacity of the TCA cycle, ketone bodies are produced. These can serve as energy substrates for the brain during starvation but may cause ketoacidosis if their concentration becomes excessive.
Ketone bodies: Acetoacetic acid, β-hydroxybutyric acid.
Ketoacidosis: Disruption of acid-base balance due to accumulation of metabolic acids.
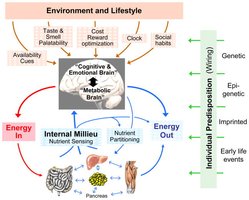
Regulation of Eating
Homeostatic vs. Non-Homeostatic Eating
Eating behavior is regulated by both homeostatic (metabolic need) and non-homeostatic (cognitive, reward, emotional) mechanisms.
Homeostatic eating: Driven by energy depletion and metabolic signals.
Non-homeostatic eating: Driven by external cues, emotions, and reward pathways; can occur in absence of hunger.
Models for Regulation of Homeostatic Eating
The hypothalamus contains centers for hunger and satiety. Two main theories explain regulation:
Glucostatic theory: Intake regulated by plasma glucose levels.
Lipostatic theory: Intake regulated by signals from fat stores (e.g., leptin).
Leptin and Appetite Regulation
Leptin is a hormone produced by adipose tissue that signals satiety and modulates eating behavior. Mutations in leptin or its receptor can lead to obesity.
Leptin deficiency: Rare, but can cause severe obesity.
Leptin resistance: Common in obesity; elevated leptin fails to suppress appetite.
Gut Signals Influencing Eating
Various gut-derived peptides regulate appetite:
Increase appetite: Ghrelin (from empty stomach).
Decrease appetite: CCK, peptide YY (PYY), GLP-1, stomach stretch and acid.

Insulin: Secretion, Action, and Diabetes Mellitus
Insulin Secretion and Regulation
Insulin is secreted by pancreatic beta cells in response to elevated plasma glucose and amino acids, as well as incretins (GLP-1, GIP) and parasympathetic stimulation.
GLUT2 transporters: Facilitate glucose entry into beta cells.
KATP channels: Close in response to increased ATP, leading to cell depolarization and insulin release.
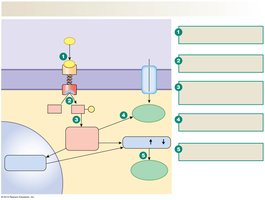
Insulin Action
Insulin promotes glucose uptake, metabolism, and storage in muscle, adipose tissue, and liver. It acts via the GLUT4 transporter in muscle and adipose, and via activation of hexokinase in hepatocytes.
Muscle and adipose: Insulin stimulates GLUT4 insertion into membrane, increasing glucose uptake.
Liver: Insulin activates hexokinase, promoting glucose storage as glycogen.
Diabetes Mellitus
Diabetes mellitus is characterized by hyperglycemia due to inadequate insulin secretion (Type 1), abnormal target cell responsiveness (Type 2), or both.
Type 1: Autoimmune destruction of beta cells; requires insulin therapy.
Type 2: Insulin resistance; often associated with obesity and metabolic syndrome.
Endocrine Response to Hypoglycemia
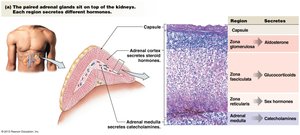
Glucagon, Cortisol, and Epinephrine
Glucagon is secreted by pancreatic alpha cells in response to low blood glucose, targeting the liver to promote glycogenolysis and gluconeogenesis. Cortisol and epinephrine also mobilize energy substrates during stress and hypoglycemia.
Glucagon: Prevents hypoglycemia by increasing hepatic glucose output.
Cortisol: Promotes gluconeogenesis, lipolysis, and proteolysis; suppresses immune response.
Epinephrine: Rapidly mobilizes energy substrates; increases glucagon, decreases insulin.

Other Hormones Affecting Metabolism
Thyroid Hormone
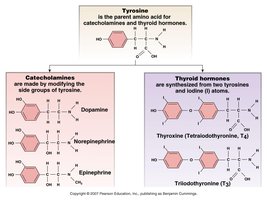
Thyroid hormones (T3 and T4) are amino acid derivatives containing iodine, essential for normal growth and development, especially of the nervous system. They increase basal metabolic rate and thermogenesis.
Hypothyroidism: Low metabolic rate, cold intolerance, goitre (often due to iodine deficiency).
Hyperthyroidism: High metabolic rate, heat intolerance, muscle weakness, exophthalmos (Graves disease).


Growth Hormone
Growth hormone (GH) is released throughout life, with major effects during childhood. It acts directly and indirectly (via insulin-like growth factors) to promote growth and metabolic changes.
Metabolic effects: Increases plasma glucose, lipolysis, and protein synthesis.
Growth effects: Stimulates cartilage, bone, muscle, and soft tissue growth.
Pathologies: Deficiency causes dwarfism; excess causes giantism or acromegaly.

Calcium Homeostasis
Calcium Functions and Distribution
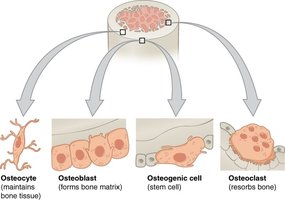
Calcium is essential for secretion, muscle contraction, blood clotting, and as a component of bone and teeth. Most calcium is stored in bone, which is continually remodeled by osteoblasts and osteoclasts.
Extracellular calcium: Involved in secretion, contraction, and clotting.
Intracellular calcium: Involved in muscle contraction and signaling.
Bone: Largest reservoir, but only a small fraction is exchangeable.
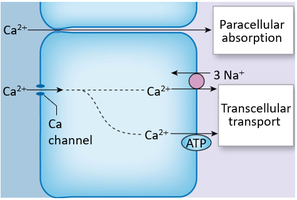
Calcium Intake and Output
Calcium is absorbed in the intestine (enhanced by vitamin D) and excreted primarily via the kidneys, with hormonally controlled reabsorption at the distal nephron.
Vitamin D and Calcium Regulation
Vitamin D is synthesized from cholesterol derivatives and is essential for calcium absorption. Its active form, calcitriol, is produced in the kidney under the influence of parathyroid hormone (PTH).
Vitamin D3 (cholecalciferol): Synthesized in skin or obtained from diet.
Calcitriol: Active form, increases calcium absorption.

Hormonal Regulation of Calcium Homeostasis
Three hormones regulate plasma calcium:
Parathyroid hormone (PTH): Released in response to hypocalcemia; increases bone resorption, kidney reabsorption, and intestinal absorption (via vitamin D).
Vitamin D3 (calcitriol): Increases calcium absorption and reabsorption.
Calcitonin: Released in response to hypercalcemia; lowers plasma calcium.
Summary Table: Hormonal Regulation of Calcium
Hormone | Stimulus | Main Actions |
|---|---|---|
Parathyroid hormone (PTH) | Low plasma Ca2+ | ↑ bone resorption, ↑ kidney reabsorption, ↑ vitamin D activation |
Vitamin D3 (calcitriol) | PTH, low plasma Ca2+ | ↑ intestinal absorption, ↑ kidney reabsorption, ↑ bone resorption |
Calcitonin | High plasma Ca2+ | ↓ bone resorption, ↓ kidney reabsorption |
Additional info: These notes expand on brief points with academic context, definitions, and examples to provide a comprehensive, exam-ready study guide for ANP college students.
