 Back
BackNutrients and Physiology of Bone Health: Study Notes for Anatomy & Physiology
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Nutrients Important for Bone Health
Bone Structure and Function
The skeletal system is essential for movement, structural support, protection of organs, blood cell synthesis, and mineral storage. Bones are living tissues that undergo continuous remodeling, adapting to mechanical stress and metabolic needs.
Movement and Support: Bones and connective tissues enable various types of movement and provide structural support.
Protection: The skeleton protects vital organs such as the brain, heart, and lungs.
Blood Cell Synthesis: Red and white blood cells and platelets are produced in bone marrow.
Mineral Storage: Bones store minerals like calcium, phosphorus, and magnesium.

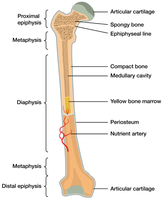
Bone Anatomy and Structure
The human skeleton consists of 206 bones, divided into the axial and appendicular skeleton. Bones are classified by shape and are composed of both inorganic and organic materials.
Axial Skeleton: Includes the skull, vertebral column, and rib cage (80 bones).
Appendicular Skeleton: Includes shoulder and pelvic girdles, and limbs (126 bones).
Bone Types: Long, short, flat, and irregular bones.
Bone Composition: About 65% mineralized matrix (hydroxyapatite, formed from calcium and phosphorus).
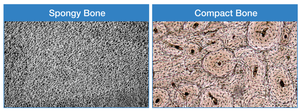
Bone Tissues: Trabecular (spongy) bone and cortical (compact) bone.
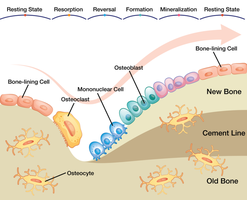
Bone Cells and Remodeling
Bones are dynamic tissues, constantly remodeled by specialized cells. Remodeling is crucial for bone health and adaptation to stress.
Osteoblasts: Build new bone tissue.
Osteoclasts: Break down bone tissue.
Osteocytes: Mature bone cells, most abundant in bone tissue.
Bone Remodeling: Involves bone resorption (osteoclasts) and bone formation (osteoblasts).
Bone Resorption: Osteoclasts secrete hydrogen ions to dissolve minerals in the bone matrix.
Osteoid: Unmineralized bone tissue.
Key Takeaways: Bone Structure and Function
The skeletal system supports movement, organ protection, blood cell synthesis, and mineral storage.
Bones are composed of periosteum, compact bone, trabecular bone, and bone marrow.
Bone remodeling is a multifaceted process requiring nutrients like calcium, phosphorus, magnesium, fluoride, vitamin D, and vitamin K.
Micronutrients Essential for Bone Health: Calcium and Vitamin D
Calcium
Calcium is the most abundant mineral in the body, vital for bone and tooth formation, nerve transmission, muscle contraction, and blood clotting.
Functions: Bone and tooth formation, nerve impulse transmission, muscle contraction, clotting factors, insulin release, glycogen breakdown, energy for muscle contraction.
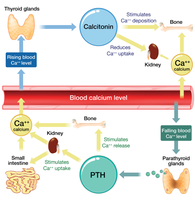
Regulation: Blood calcium is regulated by parathyroid hormone (PTH), calcitriol (active vitamin D), and calcitonin.
Sources: Dairy products, fortified foods, tofu, green vegetables.
Health Benefits: Decreases colon cancer risk, blood pressure, and kidney stone formation.
Vitamin D
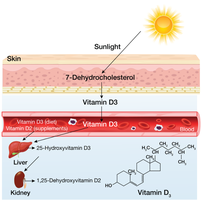
Vitamin D is a fat-soluble vitamin essential for calcium absorption and bone health. Most vitamin D3 is synthesized in the skin via sunlight exposure.
Activation: Sunlight converts 7-dehydroxycholesterol in skin to vitamin D3, which is then activated in the liver and kidneys to calcitriol.
Functions: Enhances calcium absorption, maintains bone mineral density, prevents rickets and osteomalacia.
Sources: Sunlight, fatty fish (e.g., salmon), fortified foods.
Key Takeaways: Calcium and Vitamin D
Calcium is essential for bone strength, nerve communication, muscle contraction, and blood clotting.
Calcium levels are controlled by PTH, calcitriol, and calcitonin.
Vitamin D is necessary for calcium absorption and bone health.
Recommended daily intake: Calcium (1,000–1,200 mg), Vitamin D (15–20 µg).
Other Essential Micronutrients for Bone Health
Phosphorus
Phosphorus is the second most abundant mineral in the body, with 85% stored in the skeleton. It is commonly added to foods for various purposes.
Functions: Structural component of bone, emulsifying agent, prevents clumping, improves texture and taste, extends shelf-life.
Sources: Widely available in processed foods.
Magnesium
Magnesium is a mineral found in bone tissue, essential for bone maintenance, enzymatic reactions, and nerve and muscle function.
Functions: Bone maintenance, ATP reactions, DNA/RNA synthesis, nerve conduction, muscle contraction.
Sources: Green leafy vegetables, fish, dairy, meats, whole grains, nuts, chocolate, coffee, hard water.

Fluoride
Fluoride is a mineral that prevents tooth decay and is part of mineralized bone tissue.
Functions: Blocks acid formation, prevents demineralization, enhances remineralization of enamel.
Sources: Fluoridated water.
Vitamin K
Vitamin K acts as a coenzyme modifying proteins important for bone health and normal blood clotting.
Sources: Green vegetables (broccoli, cabbage, kale, parsley, spinach, lettuce).
Key Takeaways: Other Micronutrients
Phosphorus is a primary mineral component of bone, regulated with calcium.
Magnesium deficiency can compromise bone health.
Fluoride benefits teeth and bones when present at recommended intake.
Vitamin K promotes bone health and normal blood clotting.
Osteoporosis
Characteristics and Measurement
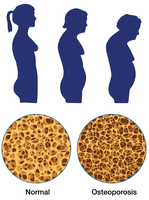
Osteoporosis is characterized by excessive bone loss, leading to weakened bones and increased fracture risk. It is measured by bone mineral density (BMD) using dual-energy X-ray absorptiometry (DEXA).
Type 1 (Postmenopausal): Occurs in women 50–70 years, rapid estrogen decline, wrist and spine fractures.
Type 2 (Senile): Occurs after age 70, affects women more, hip and spine fractures.
Peak Bone Mass: Greatest bone tissue developed in lifetime; declines after age 40.
BMD: Amount of calcified tissue per unit area; predicts fracture risk.

Key Takeaways: Osteoporosis
BMD is an indicator of bone quality and strength.
Excessive bone loss leads to osteopenia and osteoporosis.
Osteoporosis is often silent until a fracture occurs.
Risk Factors for Osteoporosis
Nonmodifiable Risk Factors
Age (after 40)
Female sex
Small body frame
White or Asian ethnicity
Low estrogen levels
Certain medications and diseases (e.g., glucocorticoids, anorexia, chronic kidney disease, Crohn’s disease, hyperthyroidism, diabetes, cancer, COPD, rheumatoid arthritis)
Modifiable Risk Factors
Physical inactivity
Being underweight
Smoking, alcohol, caffeine
Poor nutrition (low calcium and vitamin D, inadequate protein)
Key Takeaways: Risk Factors
Nonmodifiable risk factors include age, sex, body frame, ethnicity, endocrine disorders, and family history.
Modifiable risk factors include lifestyle choices and nutrition.
Dietary inadequacy, certain medications, and diseases increase osteoporosis risk.
Osteoporosis Prevention and Treatment
Primary Prevention
Building peak bone mass early in life is crucial. Prevention strategies include adequate nutrition, physical activity, and fall prevention.
Nutrition: Adequate calcium and vitamins A, C, D, E, K.
Physical Activity: Weight-bearing exercises (walking, running, sports).
Fall Prevention: Environmental modifications, vision and balance checks.
BMD Measurement: Recommended for at-risk groups (older adults, postmenopausal women, those with fractures).
Secondary Prevention
Pyramid Approach: Base level: nutrition, activity, fall prevention; second level: treat underlying disorders; third level: pharmacotherapy.
Key Takeaways: Prevention and Treatment
Primary prevention starts early with diet and exercise.
Secondary prevention aims to arrest bone loss and reduce fracture risk.
Three-tiered approach: lifestyle, assessment/treatment of causes, pharmacotherapy.
Deficiency, Supplementation, and Choices
Groups at Risk for Calcium Inadequacy
Adolescent teens (reduced dairy consumption)
Women with amenorrhea (low estrogen)
Female athlete triad (amenorrhea, disrupted eating, osteoporosis)
Older adults (reduced calcium bioavailability)
Postmenopausal women (decline of estrogen)
Lactose-intolerant people
Vegans (plant-based diets with oxalates/phytates, avoid dairy)
Calcium Supplements
Types: Calcium carbonate, citrate, lactate, phosphate (about 200 mg elemental calcium per pill).
Some natural sources (oyster shell, bone meal, dolomite) may contain high lead levels.
Benefits: Increased peak bone mass, maintained BMD, reduced osteoporosis risk, decreased fracture incidence (when taken with vitamin D).
GI tract can only absorb up to 500 mg calcium at a time; split doses are more effective.
The Calcium Debate
Sufficient dietary calcium prevents osteoporosis and cardiovascular disease.
Supplements advised for those unable to meet dietary needs.
Excess calcium can impair absorption of other minerals (iron, zinc).
Other Choices Affecting Bone Health
High phosphate (from soda) decreases bone health.
Lactose-free diets may predispose to inadequate bone mineralization.
Key Takeaways: Deficiency and Supplementation
At-risk groups: teens, amenorrheic women, female athletes, older adults, lactose-intolerant, vegans.
Monitor vitamin D intake with calcium supplements; split doses for better absorption.
Best calcium sources are dietary; supplementation is beneficial when needed.
