 Back
BackStudy Guide: Bones, Joints, and Muscle Tissue (Chapters 6, 8, 9)
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Chapter 6: Bones and Skeletal Tissues
6.1 Skeletal Cartilages: Structure, Types, and Growth
Skeletal cartilages provide flexible support and resilience to the body. They are surrounded by the perichondrium, a dense irregular connective tissue that resists outward expansion and contains blood vessels for nutrient delivery.
Hyaline cartilage: Most abundant; found in articular, costal, respiratory, and nasal cartilages. Provides support with flexibility and resilience.
Elastic cartilage: More flexible than hyaline; found in the external ear and epiglottis.
Fibrocartilage: Highly compressible with great tensile strength; found in knee menisci and intervertebral discs.
Cartilage grows by two mechanisms:
Appositional growth: Cells in the perichondrium secrete new matrix on the external surface.
Interstitial growth: Chondrocytes within the cartilage divide and secrete new matrix, expanding the cartilage from within.
6.2 Functions of Bones
Bones perform several essential functions for the body:
Support: Framework for the body and soft organs.
Protection: Enclose and protect vital organs (e.g., brain, heart).
Anchorage: Skeletal muscles attach to bones via tendons for movement.
Mineral storage: Reservoir for calcium and phosphate.
Blood cell formation: Hematopoiesis in red marrow cavities.
Triglyceride storage: Fat storage in yellow marrow.
Hormone production: Osteocalcin regulates insulin and energy metabolism.
6.3 Classification of Bones
Bones are classified by location and shape:
Axial skeleton: Skull, vertebral column, rib cage (protection, support).
Appendicular skeleton: Limbs and girdles (movement, manipulation).
Bone shapes:
Long bones: Longer than wide (e.g., femur, humerus).
Short bones: Cube-shaped (e.g., carpals, tarsals).
Flat bones: Thin, often curved (e.g., sternum, skull bones).
Irregular bones: Complicated shapes (e.g., vertebrae, hip bones).
6.4 Bone Structure and Composition
All bones have an outer layer of compact bone and inner spongy bone (trabeculae). Key structures include:
Diaphysis: Shaft of long bone, contains medullary cavity (yellow marrow in adults).
Epiphyses: Bone ends, contain spongy bone and red marrow.
Periosteum: Outer membrane with osteogenic cells.
Endosteum: Internal membrane lining medullary cavity and trabeculae.
Bone markings: Projections (muscle/ligament attachment), surfaces (joints), depressions/openings (passage for vessels/nerves).
Microscopically, bone contains:
Osteoprogenitor cells: Stem cells.
Osteoblasts: Bone-forming cells.
Osteocytes: Mature bone cells maintaining matrix.
Osteoclasts: Bone-resorbing cells.
Chemical composition:
Organic: Cells and osteoid (collagen fibers, ground substance) for flexibility.
Inorganic: Hydroxyapatites (calcium phosphates) for hardness and strength.
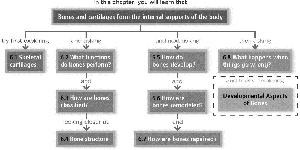
6.5 Bone Development (Ossification)
Bone formation (ossification) occurs by two processes:
Endochondral ossification: Bone replaces hyaline cartilage (all bones below skull except clavicles).
Intramembranous ossification: Bone develops from fibrous membranes (cranial bones, clavicles).
Longitudinal growth occurs at the epiphyseal plate through zones of resting, proliferation, hypertrophy, calcification, and ossification. Appositional growth increases bone thickness.
6.6 Bone Remodeling
Bone remodeling is a continuous process involving bone deposition (by osteoblasts) and resorption (by osteoclasts). It is regulated by:
Hormones: Parathyroid hormone (PTH) increases blood calcium by stimulating osteoclasts; calcitonin lowers blood calcium.
Mechanical stress: Wolff’s law states bone adapts to the loads under which it is placed.
6.7 Bone Repair
Bone fracture repair involves four stages:
Hematoma formation
Fibrocartilaginous callus formation
Bony callus formation
Bone remodeling
6.8 Bone Disorders
Osteomalacia/Rickets: Poor mineralization, soft bones (adults/children).
Osteoporosis: Bone resorption exceeds formation; porous, fragile bones.
Paget’s disease: Excessive, disorganized bone remodeling.
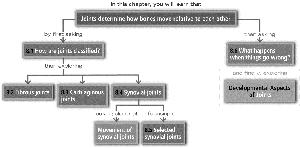
Chapter 8: Joints
8.1 Classification of Joints
Joints (articulations) are classified by structure and function:
Structural: Fibrous, cartilaginous, synovial (based on binding material and presence of cavity).
Functional: Synarthroses (immovable), amphiarthroses (slightly movable), diarthroses (freely movable).
8.2 Fibrous Joints
Sutures: Immovable, found in skull.
Syndesmoses: Bones connected by ligaments (e.g., distal tibiofibular joint).
Gomphoses: Peg-in-socket (e.g., teeth in alveolar sockets).
8.3 Cartilaginous Joints
Synchondroses: Bones united by hyaline cartilage (e.g., epiphyseal plate).
Symphyses: Bones united by fibrocartilage (e.g., intervertebral discs, pubic symphysis).
8.4 Synovial Joints
Synovial joints are freely movable and have a fluid-filled cavity. Key features:
Articular cartilage, joint cavity, articular capsule, synovial fluid, reinforcing ligaments, nerves, and blood vessels.
Bursae and tendon sheaths reduce friction.
Stability depends on articular surfaces, ligaments, and muscle tone.
Movements include gliding, angular (flexion, extension, abduction, adduction, circumduction), rotation, and special movements (supination, pronation, opposition, dorsiflexion, plantar flexion, inversion, eversion, elevation, depression, protraction, retraction).
Types of synovial joints: plane, hinge, pivot, condylar, saddle, ball-and-socket.
8.5 Examples of Synovial Joints
Temporomandibular joint (TMJ): Hinge and gliding movements.
Shoulder: Ball-and-socket, most mobile, least stable.
Elbow: Hinge joint, flexion/extension.
Hip: Ball-and-socket, deep socket for stability.
Knee: Largest, three joints in one, hinge with some rotation.
8.6 Joint Injuries and Disorders
Injuries: Cartilage tears, sprains, dislocations.
Inflammatory/degenerative conditions: Bursitis, tendonitis, arthritis (osteoarthritis, rheumatoid arthritis, gouty arthritis), Lyme disease.
Chapter 9: Muscles and Muscle Tissue
9.1 Types and Functions of Muscle Tissue
There are three types of muscle tissue:
Skeletal muscle: Striated, voluntary, attached to bones.
Cardiac muscle: Striated, involuntary, found in heart.
Smooth muscle: Non-striated, involuntary, found in walls of hollow organs.
Functions: movement, posture maintenance, joint stabilization, heat generation.
9.2 Structure of Skeletal Muscle
Composed of muscle fibers, nerves, blood vessels, and connective tissue sheaths (epimysium, perimysium, endomysium).
Muscles attach to bones directly (epimysium to periosteum) or indirectly (via tendons or aponeuroses).
9.3 Microscopic Anatomy of Skeletal Muscle
Myofibrils: Contain contractile elements (sarcomeres) with thick (myosin) and thin (actin) filaments.
Sarcoplasmic reticulum (SR): Stores and releases calcium ions.
T tubules: Conduct impulses to deep regions of muscle fiber.
Sliding filament model: Thin filaments slide past thick filaments, shortening the sarcomere during contraction.
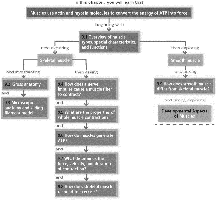
9.4 Muscle Contraction: Neuromuscular Junction and Excitation-Contraction Coupling
Motor neurons release acetylcholine (ACh) at the neuromuscular junction, triggering an action potential in the muscle fiber.
Action potential travels along sarcolemma and T tubules, causing SR to release calcium.
Calcium binds to troponin, moving tropomyosin and exposing myosin-binding sites on actin.
Cross-bridge cycling occurs, resulting in muscle contraction.
9.5 Muscle Twitch, Summation, and Contraction Types
Motor unit: One motor neuron and all muscle fibers it innervates.
Muscle twitch: Response to a single stimulus (latent, contraction, relaxation phases).
Summation: Increased frequency or strength of stimulation increases contraction force.
Isotonic contractions: Muscle changes length (concentric/eccentric).
Isometric contractions: Muscle tension increases, but length does not change.
9.6 ATP Production and Muscle Fatigue
ATP is regenerated by direct phosphorylation (creatine phosphate), anaerobic glycolysis, and aerobic respiration.
Muscle fatigue: Inability to contract due to ionic imbalances, decreased ATP, or other factors.
Excess postexercise oxygen consumption (EPOC): Oxygen needed to restore muscle to resting state.
9.7 Factors Affecting Muscle Contraction
Force depends on frequency of stimulation, number and size of fibers recruited, and degree of muscle stretch.
Velocity and duration depend on muscle fiber type (slow oxidative, fast glycolytic, fast oxidative), load, and recruitment.
9.8 Muscle Response to Exercise
Aerobic exercise: Increases endurance, capillaries, mitochondria, myoglobin.
Resistance exercise: Increases muscle size (hypertrophy), strength, and glycogen storage.
9.9 Smooth Muscle
Non-striated, involuntary, found in hollow organs.
Contracts via sliding filament mechanism, but lacks sarcomeres and troponin (uses calmodulin).
Can be unitary (visceral) or multi-unit (independent fibers).
Developmental Aspects
Muscle and bone tissues develop from mesodermal cells (myoblasts for muscle, mesenchymal cells for bone).
Growth and regeneration capacity varies by tissue type and age.
