 Back
BackThe Urinary System: Structure, Function, and Physiology
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
The Urinary System
Overview and Importance
The urinary system is essential for maintaining the body's internal environment by regulating water, solute concentrations, and removing metabolic wastes. Understanding its function is crucial for diagnosing and managing renal diseases.
Main organs: Kidneys, ureters, urinary bladder, urethra
Primary functions: Excretion of wastes, regulation of water and electrolytes, acid-base balance, hormone production (erythropoietin, renin), activation of vitamin D, and gluconeogenesis during prolonged fasting.
Gross Anatomy of the Kidneys
Location and External Anatomy
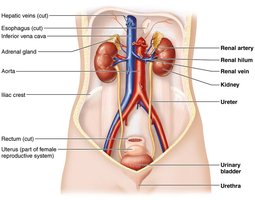
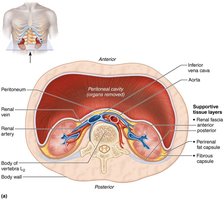
The kidneys are retroperitoneal organs located in the superior lumbar region, between T12 and L5 vertebrae. The right kidney is slightly lower due to the liver. Each kidney is capped by an adrenal gland and has a convex lateral surface and a concave medial surface with a renal hilum for entry/exit of vessels and nerves.
Supportive tissue layers:
Renal fascia: outer dense connective tissue
Perirenal fat capsule: cushioning fat layer
Fibrous capsule: transparent layer preventing infection spread

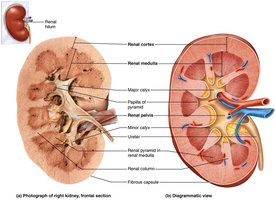
Internal Gross Anatomy
Internally, the kidney has three main regions: cortex, medulla, and pelvis. The medulla contains renal pyramids separated by renal columns. The renal pelvis collects urine from major and minor calyces and channels it to the ureter.
Urine flow: Renal pyramid → minor calyx → major calyx → renal pelvis → ureter
Blood and Nerve Supply
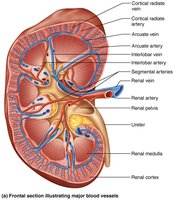
The kidneys receive about 25% of cardiac output via the renal arteries. Blood flows through a series of arteries and veins, with no segmental veins. Sympathetic nerves regulate renal blood flow and renin release.
Arterial flow: Renal → segmental → interlobar → arcuate → cortical radiate
Venous flow: Cortical radiate → arcuate → interlobar → renal veins

Nephrons: Structure and Function
Overview
Nephrons are the functional units of the kidney, responsible for urine formation. Each kidney contains over one million nephrons, each consisting of a renal corpuscle and a renal tubule.
Renal corpuscle: Glomerulus (capillary tuft) + glomerular (Bowman's) capsule
Renal tubule: Proximal convoluted tubule (PCT), nephron loop (loop of Henle), distal convoluted tubule (DCT)

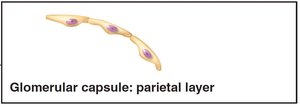
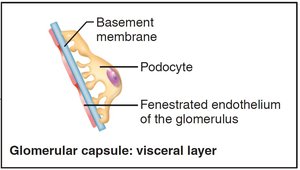
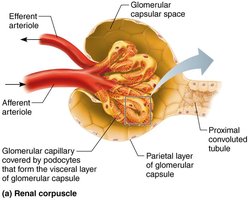
Renal Corpuscle
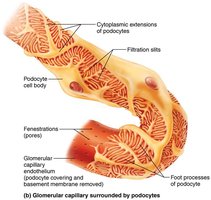
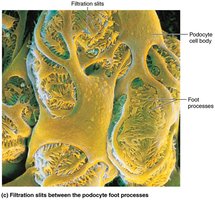
The renal corpuscle filters blood plasma. The glomerulus is a fenestrated capillary network, and the surrounding capsule has parietal and visceral layers. Podocytes in the visceral layer form filtration slits.
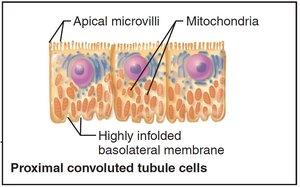
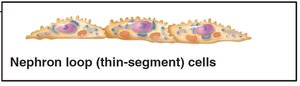
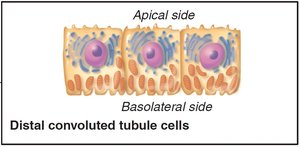
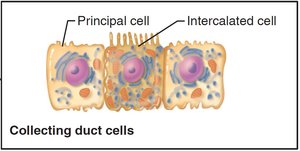
Renal Tubule and Collecting Duct
The renal tubule processes filtrate through reabsorption and secretion. The PCT is specialized for reabsorption, the nephron loop for creating osmotic gradients, and the DCT for regulated secretion and reabsorption. Collecting ducts receive filtrate from multiple nephrons and help concentrate urine.

Types of Nephrons
Cortical nephrons: 85% of nephrons, mostly in cortex
Juxtamedullary nephrons: Long loops extend deep into medulla, crucial for concentrated urine production

Nephron Capillary Beds
Glomerulus: Specialized for filtration, fed and drained by arterioles
Peritubular capillaries: Adapted for absorption, surround cortical nephrons
Vasa recta: Surround juxtamedullary nephrons, maintain medullary osmotic gradient


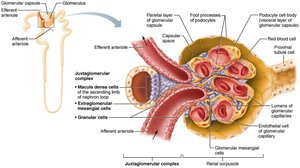
Juxtaglomerular Complex (JGC)
The JGC regulates filtrate formation and blood pressure. It includes macula densa (chemoreceptors), granular cells (mechanoreceptors, secrete renin), and extraglomerular mesangial cells (signal transmission).
Physiology of the Kidney
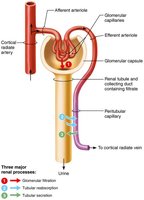
Urine Formation
The kidneys process about 180 L of fluid daily, forming 1.5 L of urine. Three main processes occur:
Glomerular filtration: Passive filtration of plasma minus proteins
Tubular reabsorption: Selective return of substances to blood
Tubular secretion: Selective addition of substances to filtrate
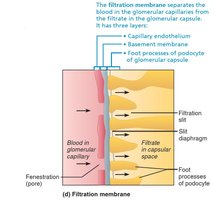
Glomerular Filtration
Filtration occurs across a three-layered membrane: fenestrated endothelium, basement membrane, and podocyte filtration slits. Only small molecules pass; proteins and cells are retained.
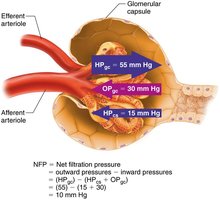
Filtration Pressures
Net filtration pressure (NFP) is determined by hydrostatic and osmotic pressures:
Outward pressure (HPgc): 55 mm Hg (glomerular blood pressure)
Inward pressures: HPcs (15 mm Hg, capsular) + OPgc (30 mm Hg, colloid osmotic)
NFP equation:
Typical value: mm Hg
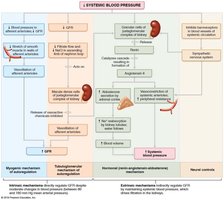
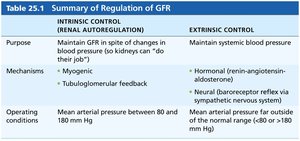
Regulation of Glomerular Filtration Rate (GFR)
GFR must be tightly regulated to maintain homeostasis. Intrinsic (renal autoregulation) and extrinsic (neural/hormonal) mechanisms adjust GFR.
Intrinsic: Myogenic and tubuloglomerular feedback mechanisms
Extrinsic: Sympathetic nervous system, renin-angiotensin-aldosterone system
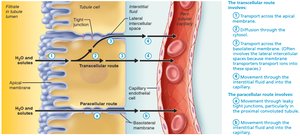
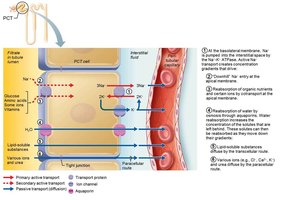
Tubular Reabsorption
Most filtrate is reabsorbed via transcellular or paracellular routes. Sodium reabsorption drives reabsorption of other solutes and water. Water follows by osmosis (obligatory and facultative reabsorption).
Transport Maximum
Each solute has a transport maximum (Tm), reflecting the number of available carriers. Excess solute is excreted in urine (e.g., glucose in diabetes).
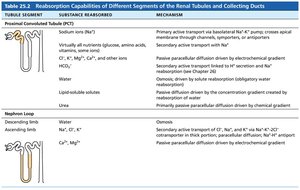
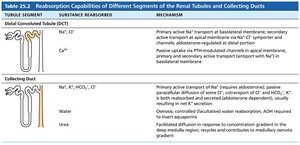
Reabsorptive Capabilities of Tubules
PCT: Site of most reabsorption (all nutrients, 65% Na+ and water)
DCT and collecting duct: Hormonally regulated (ADH, aldosterone, ANP, PTH)

Tubular Secretion
Secretion removes additional wastes (K+, H+, NH4+, creatinine, drugs) from blood into filtrate, mainly in the PCT.


Regulation of Urine Concentration and Volume
Countercurrent Mechanisms
Countercurrent multiplier (nephron loop) and exchanger (vasa recta) establish and maintain a medullary osmotic gradient, allowing the kidney to produce urine of varying concentration (300–1200 mOsm).






Urea Recycling
Urea contributes to the medullary osmotic gradient by recycling between the collecting duct and nephron loop.
Clinical Evaluation of Kidney Function
Urinalysis and Renal Clearance
Urinalysis detects disease; renal clearance tests measure GFR and kidney function. Inulin is the standard for GFR measurement.
Renal clearance equation:
C = clearance rate (ml/min), U = urine concentration, V = urine flow rate, P = plasma concentration
Clinical Disorders
Chronic renal disease: GFR < 60 ml/min for 3 months
Renal failure: GFR < 15 ml/min, requires dialysis or transplant
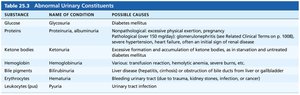
Urine Composition and Characteristics
Chemical composition: 95% water, 5% solutes (urea, uric acid, creatinine, ions)
Physical characteristics: Clear, pale to deep yellow, slightly aromatic, pH ~6, specific gravity 1.001–1.035
Transport, Storage, and Elimination of Urine
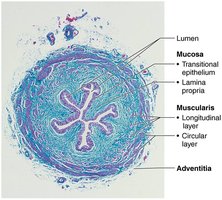
Ureters
Ureters are muscular tubes that transport urine from kidneys to bladder. They have mucosa, muscularis, and adventitia layers.
Urinary Bladder
The bladder is a muscular sac for temporary urine storage, with a trigone region prone to infection. The wall has mucosa, detrusor muscle, and adventitia.
Urethra
The urethra drains urine from the bladder. It has internal (involuntary) and external (voluntary) sphincters. Male and female urethras differ in length and function.
Micturition (Urination)
Micturition involves detrusor contraction, internal sphincter opening (ANS), and external sphincter relaxation (somatic nervous system). Reflexive urination is present in infants; voluntary control develops with age.
Developmental and Clinical Aspects
Embryonic development: Kidneys develop from pronephros, mesonephros, and metanephros stages.
Congenital abnormalities: Horseshoe kidney, hypospadias, polycystic kidney disease
Aging: Kidney function declines with age; incontinence and nocturia are common in elderly.
