 Back
BackProtein Therapeutics: Biochemistry Study Guide
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Protein Therapeutics
Overview of Protein Therapies
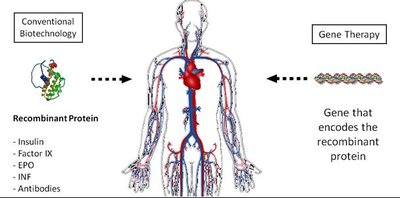
Protein therapeutics are engineered proteins used in medicine to treat diseases, alleviate symptoms, or repair biological structures. These proteins are administered in precise amounts and are often produced using recombinant DNA technology.
Definition: Therapeutic proteins are laboratory-engineered proteins for pharmaceutical use.
Applications: Used to treat illnesses, pain, and structural repair.
Production: Most are recombinant proteins, produced using genetic engineering.

Advantages and Disadvantages of Protein Therapies
Protein therapies offer several benefits over traditional small molecule drugs, but also present unique challenges.
Advantages:
Highly specific and selective
Low toxicity and fewer side effects
Low tissue accumulation
High biological and chemical diversity
Disadvantages:
Metabolic instability
Poor membrane permeability
Poor oral bioavailability
Poor solubility
Rapid clearance from the body
High manufacturing and quality assurance costs
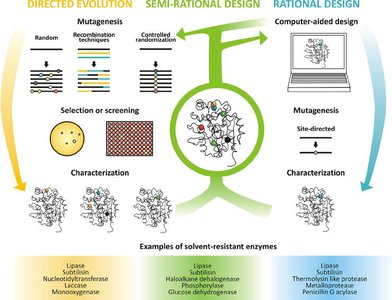
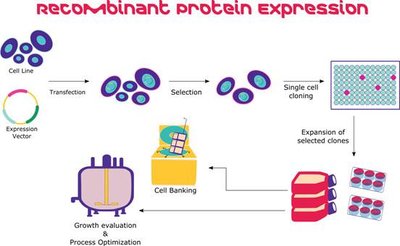
Protein Engineering and Recombinant DNA Technology
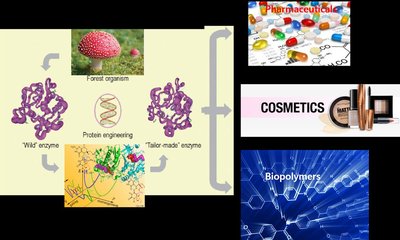
Protein engineering involves modifying proteins to enhance their properties for therapeutic use. Recombinant DNA technology enables the production of these proteins in host cells.
Protein Engineering: Altering protein structure/function for improved efficacy.
Recombinant DNA Technology: Inserting genes encoding therapeutic proteins into host cells for expression.

Timeline of Protein Therapeutics Development
The development of protein therapeutics has evolved rapidly since the early 20th century, with milestones including the use of insulin, growth hormone, and monoclonal antibodies.
1920s: Insulin therapy introduced
1982: Recombinant human insulin approved
1985: Recombinant growth hormone manufactured
1997: First chimeric and humanized antibodies approved
1998: First fusion protein approved
Classification of Protein Therapies
Protein therapeutics are classified based on their mechanism and application:
Group I: Enzymatic or regulatory activity
Ia: Replacement of deficient/abnormal protein
Ib: Augmentation of existing pathway
Ic: Provision of novel function/activity
Group II: Special targeting activity
IIa: Interference with molecules/organisms
IIb: Delivery of compounds/proteins
Group III: Protein vaccines
IIIa: Protection against foreign agents
IIIb: Treatment of autoimmune disease
IIIc: Cancer treatment
Group IV: Protein diagnostics
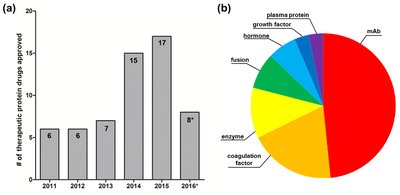
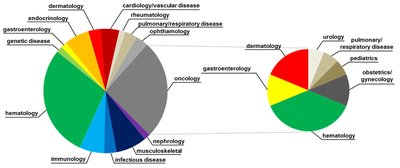
Distribution and Complexity of Therapeutic Proteins
Monoclonal antibodies constitute nearly half of approved protein therapies.
Therapeutic proteins are used across diverse medical fields, including oncology, immunology, and endocrinology.
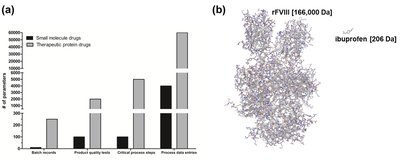
Protein drugs are more complex and costly to manufacture than small molecule drugs.
Case Study: Alpha-1 Antitrypsin (Aralast/Prolastin)
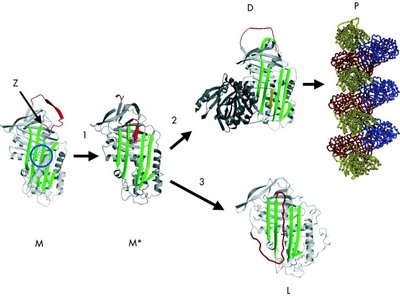
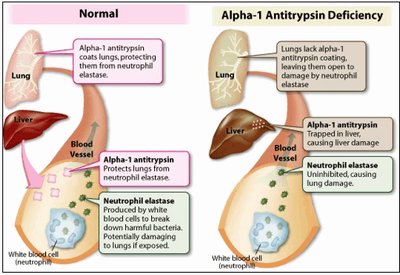
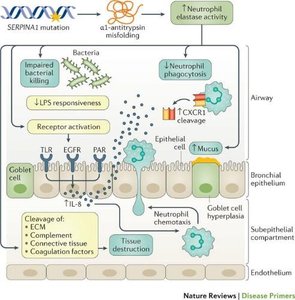
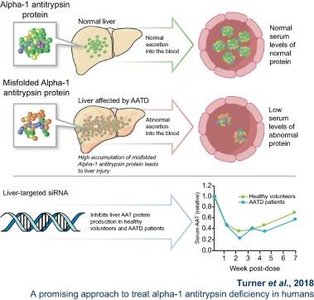
Alpha-1 Antitrypsin Deficiency
Alpha-1 antitrypsin (AAT) is a protein that inhibits elastase, a protease active in lung tissue. Deficiency in AAT leads to lung and liver disease.
Genetic Basis: Autosomal recessive disorder caused by mutations in the SERPINA1 gene.
Clinical Manifestations:
Liver cirrhosis due to misfolded AAT trapped in the liver
Emphysema due to unregulated elastase activity in the lungs
Therapeutic Approach: Replacement therapy with purified or recombinant AAT.

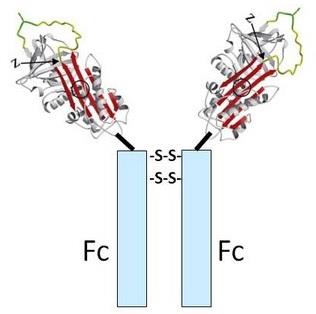
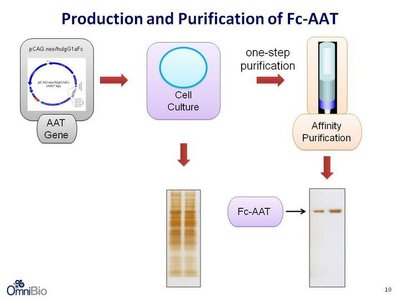
Alpha-1 Antitrypsin Therapy and Recombinant Fc-AAT
Traditional Therapy: Plasma-derived AAT, expensive and risk of contamination.
Recombinant Fc-AAT: Fusion protein with Fc region for improved stability and purification.
Benefits: Higher potency, easier purification, reduced cost, improved patient outcomes.
Case Study: TNKase (Tenecteplase)
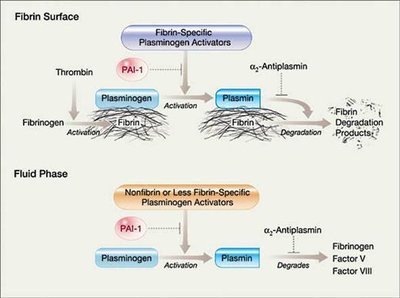
TNKase and the Fibrinolytic System
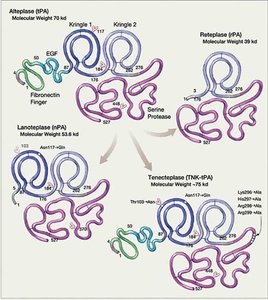
TNKase is a genetically engineered tissue plasminogen activator (tPA) used to dissolve blood clots, especially in acute myocardial infarction.
Mechanism: Converts plasminogen to plasmin, which degrades fibrin in blood clots.
Therapeutic Class: Group I, Ib: Augmenting an existing pathway.
Production: Recombinant protein produced in CHO cells.


Structural Modifications of TNKase
TNKase is a modified version of alteplase with enhanced properties:
T103N: Adds glycosylation site
N117Q: Removes glycosylation site
K296, H297, R298, R299: Replaced by alanine for enhanced fibrin specificity and resistance to PAI-1 inhibition
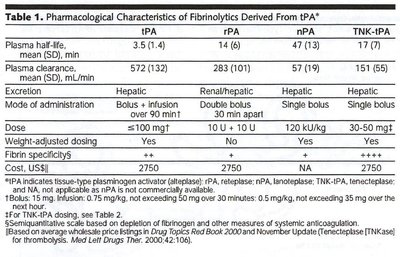
Longer half-life and single-dose administration

Case Study: Pulmozyme (Dornase Alfa)
Pulmozyme and Cystic Fibrosis
Pulmozyme is a recombinant human deoxyribonuclease 1 (DNase I) used to treat cystic fibrosis by degrading extracellular DNA in pulmonary secretions.
Mechanism: Hydrolyzes DNA in mucus, reducing viscosity and promoting clearance.
Clinical Use: Reduces respiratory infections and improves lung function in cystic fibrosis patients.
Production: Recombinant protein produced in CHO cells.
Cystic Fibrosis Pathophysiology
Genetic Basis: Autosomal recessive mutations in the CFTR gene.
Manifestations: Thick, viscous pulmonary secretions, frequent infections, reduced lung function.
Common Mutations: G551D (defective channel), F508del (misfolded protein).
Pulmozyme Administration
Administered as an aerosol mist via nebulizer.
Thins pulmonary secretions, reduces infection risk, improves lung function.
Summary: Key Concepts in Protein Therapeutics
Understanding the classification and mechanism of protein therapies
Advantages and limitations compared to small molecule drugs
Examples of protein therapies, including recombinant proteins and their modifications
Pathophysiology of diseases treated by protein therapeutics
Production and administration methods for therapeutic proteins
Additional info: Academic context was added to clarify mechanisms, genetic basis, and therapeutic approaches for each protein therapy example.
