 Back
BackIncome Inequality, Work Precarity, and Health: Social Determinants in Canada
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Income Inequality and Health in Canada
Overview of Income Distribution
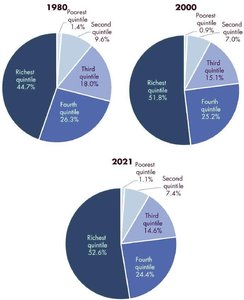
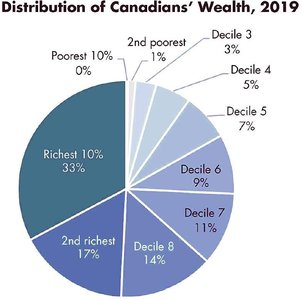
Income inequality refers to the uneven distribution of income and wealth within a society, resulting in disparities between the richest and poorest groups. In Canada, income and wealth have become increasingly concentrated among the wealthiest segments over the past four decades.
Key Terms: Quintiles divide the population into five equal groups by income; deciles divide into ten groups.
Trends: The share of total income held by the richest quintile has grown, while the poorest quintiles have seen their share shrink.
Measuring Income Inequality
Several tools are used to measure income inequality:
Lorenz Curve: A graphical representation of income distribution. The further the curve is from the diagonal (perfect equality), the greater the inequality.
Gini Index: A numerical measure (0 = perfect equality, 1 = perfect inequality) derived from the Lorenz curve.
Decile/Quintile Ratios: Compare the income of the richest to the poorest segments.
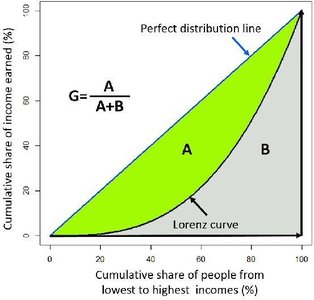
Formula for Gini Index:
Groups Most Affected by Inequality
Poorest Canadians: Minimum wage often below poverty line.
Children: 1 in 10 live in poverty; rates higher for Indigenous children.
Racialized & Indigenous persons: Earn significantly less than white Canadians; higher poverty risk.
Women: Persistent gender pay gap; "ceiling effect" limits income even at high levels.
Persons with Disabilities: Higher poverty rates, especially for severe disabilities.
Geography: Rural and certain provinces have lower incomes.
Health and Social Effects of High Inequality
High income inequality is associated with:
Poorer mental and physical health
Reduced life expectancy
Increased crime rates
Root Causes: Linked to uneven distribution of power, privilege, and prestige, intersecting with systemic racism, sexism, ableism, and colonial legacies.
Income and Health: Theoretical Models
Social Determinants of Health (SDOH)
The SDOH are the conditions in which people are born, live, grow, work, and age. Income is the most powerful SDOH, with a strong correlation to health outcomes and a clear social gradient: lower income is associated with poorer health.
Models Explaining the Income-Health Link
Behavioural Model: Health behaviours (diet, smoking, exercise) differ by income, but these "choices" are shaped by structural inequality.
Psychosocial Model: Stress from subordination and marginalization harms health by affecting the body's susceptibility to disease.
Materialist Model: Income directly determines access to resources like safe housing, education, and healthcare.
Lifecourse Model: Long-term accumulation of risks damages health over time.
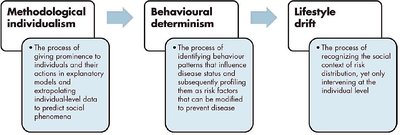
Methodological Individualism, Behavioural Determinism, and Lifestyle Drift
There is a tendency in health policy to focus on individual behaviours rather than addressing upstream social causes of health inequities.
Case Study: Income and Lung Cancer
Income-Based Disparities in Lung Cancer
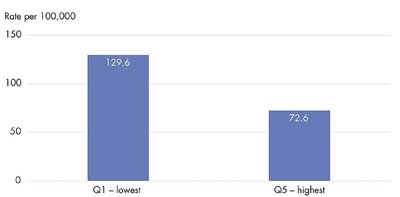
Lung cancer is the leading cause of cancer death in Canada. Income-based disparities are evident in incidence, risk factors, stage at diagnosis, treatment, and survival.
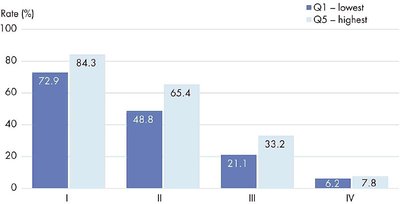
Incidence: Low-income individuals are twice as likely to be diagnosed with lung cancer.
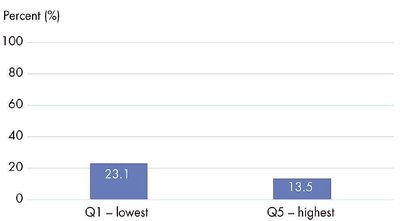
Risk Factors: Smoking rates are higher in low-income groups.
Stage at Diagnosis: Poorer individuals are more likely to be diagnosed at a late stage.
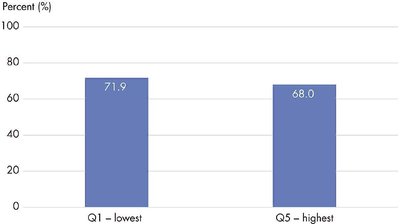
Treatment: Wealthier patients are more likely to receive curative surgery.
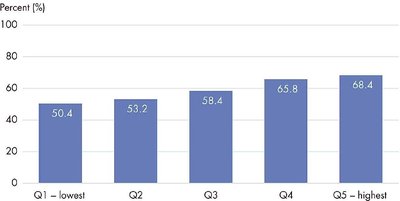
Survival: Poorer patients have lower survival rates.
Policy and Practice Implications
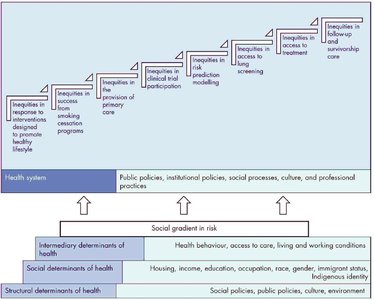
Inequities are shaped by poor distribution of SDOH (e.g., smoking, occupational hazards, environmental exposures).
Health system design can perpetuate inequities if it excludes vulnerable groups.
Equity-first approaches require co-creation with affected groups and action on upstream determinants, not just downstream interventions.
Work, Precarity, and Health
Work as a Social Determinant of Health
Work and employment are fundamental social determinants of health. Labour market insecurity, precarious employment, and workplace hazards all influence health outcomes.
Labour Market Insecurity: Includes unemployment, underemployment, and non-standard work (part-time, contract, gig work).
Precarious Employment: Characterized by instability, lack of benefits, and low job security.
Dimensions of Labour Market Security
Employment Security: Stability in accessing paid work.
Job Security: Protection from dismissal and stability in position.
Income Security: Adequacy and predictability of income.
Work Security: Protection from unsafe or unhealthy conditions.
Declines in these securities since the 1980s have led to increased precarity and negative health outcomes, especially for racialized workers, youth, and women.
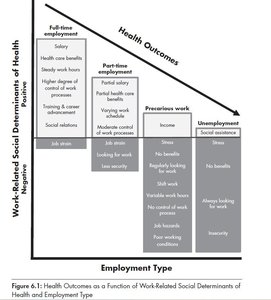
Health Impacts of Precarious Work
Precarious workers experience higher stress, poorer working conditions, and worse health outcomes.
Financial strain from income insecurity leads to depression and anxiety.
Secure jobs are associated with the best health outcomes; precarious and unemployed workers have the worst.
Summary Table: Income, Work, and Health
Factor | Impact on Health |
|---|---|
Low Income | Poorer health, higher disease rates, lower life expectancy |
Income Inequality | Increased social problems, reduced well-being |
Precarious Work | Higher stress, worse health outcomes |
Secure Employment | Better health, stability, and well-being |
Conclusion
Income and work are core social determinants of health. Addressing health inequities requires action on upstream social and economic factors, not just individual behaviours. Policies that promote equity, job security, and fair distribution of resources are essential for improving population health.
