 Back
BackSocial Determinants of Health: Mechanisms, Pathways, and Inequality
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Social Determinants of Health: Concepts and Frameworks
Introduction to Social Determinants of Health (SDOH)
The social determinants of health (SDOH) are the non-medical factors that influence health outcomes. These include the conditions in which people are born, grow, live, work, and age, as well as the broader set of forces and systems shaping the conditions of daily life. SDOH are primary predictors of health outcomes, often outweighing the effects of individual behaviors such as smoking or diet.
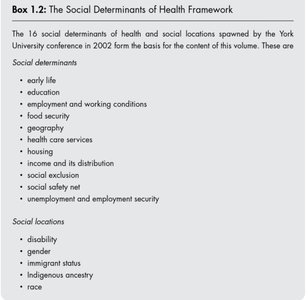
Key SDOH: Early life, education, employment and working conditions, food security, geography, health care services, housing, income and its distribution, social exclusion, social safety net, unemployment and employment security.
Social Locations: Disability, gender, immigrant status, Indigenous ancestry, race.
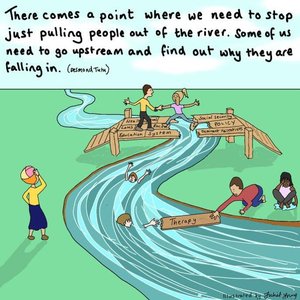
Upstream vs. Downstream Approaches
Addressing health requires moving beyond treating individual cases ('pulling people out of the river') to addressing root causes ('going upstream'). Upstream interventions focus on changing social, economic, and policy environments to prevent health problems before they occur.
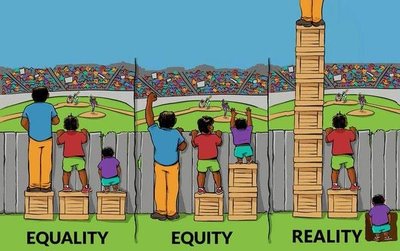
Equality, Equity, and Reality in Health
Understanding the difference between equality (everyone gets the same resources), equity (resources are distributed based on need), and reality (systemic barriers persist) is crucial for addressing health disparities. True health equity requires removing structural barriers, not just equalizing resources.
Mechanisms and Pathways: How SDOH Affect Health
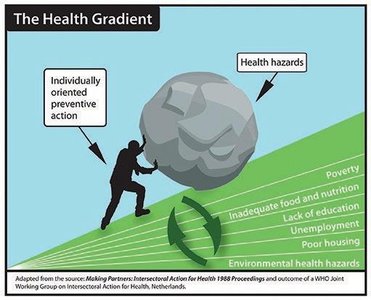
The Health Gradient
The health gradient illustrates how health outcomes improve with each step up the social ladder. Factors such as poverty, inadequate nutrition, lack of education, unemployment, and poor housing create cumulative health hazards that cannot be overcome by individual action alone.
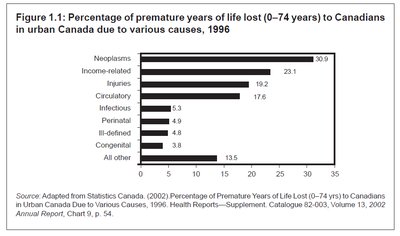
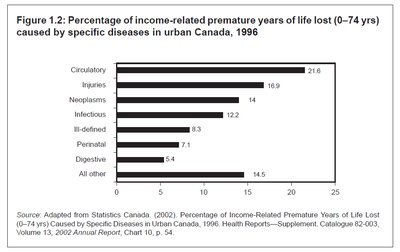
Premature Mortality and Income Inequality
Income-related factors are a major cause of premature years of life lost in Canada. Diseases such as cardiovascular disease, cancers, and injuries are disproportionately higher among those with lower income.
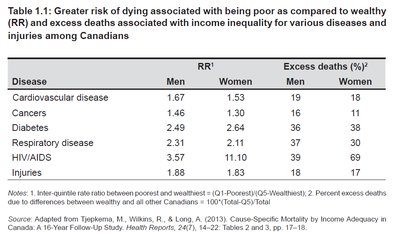
Relative Risk and Excess Deaths
Being poor is associated with a higher relative risk (RR) of dying from major diseases compared to being wealthy. The table below summarizes the RR and excess deaths for various diseases among Canadians.
Disease | RR1 Men | RR1 Women | Excess deaths (%) Men | Excess deaths (%) Women |
|---|---|---|---|---|
Cardiovascular disease | 1.67 | 1.53 | 19 | 18 |
Cancers | 1.46 | 1.30 | 16 | 11 |
Diabetes | 2.49 | 2.64 | 21 | 26 |
Respiratory disease | 2.31 | 2.11 | 37 | 39 |
HIV/AIDS | 3.57 | 11.40 | 18 | 30 |
Injuries | 1.88 | 1.83 | 17 | 17 |
International Comparisons and Child Well-Being
OECD Rankings and Child Health
International comparisons show that countries with stronger social policies and lower inequality (e.g., Finland, Netherlands) have better health outcomes and child well-being. Canada performs well in academic skills but lags in mental health and equity.

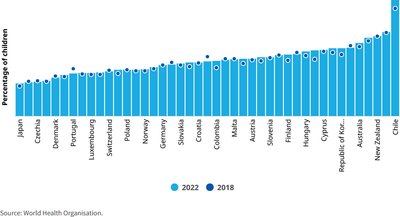
Trends in Child Well-Being
Recent UNICEF reports highlight declining life satisfaction and rising mental health challenges among children in wealthy nations, including Canada. Overweight rates and suicide risks remain persistent issues, reflecting the ongoing impact of material and social stressors.
Frameworks for Understanding SDOH
Materialist and Neo-Materialist Frameworks
Materialist frameworks focus on how objective living conditions (e.g., income, housing, employment) shape health. Neo-materialist perspectives emphasize the role of societal resource distribution and public investment in creating health equity.
Material advantage/disadvantage across the life course predicts health outcomes.
Health gradient: Stepwise differences in health by socioeconomic position.
Neo-materialist view: Societies with more equal distribution of resources and stronger public services have healthier populations.
Psychobiological Stress Response
Chronic stress from social disadvantage leads to allostatic load—the cumulative wear and tear on the body. This increases risks for cardiovascular disease, diabetes, and premature death.
Allostasis: The body's ability to maintain stability through change.
Allostatic load: Damage from repeated or prolonged stress responses.
Lifecourse Perspective
Health is shaped by early life experiences and accumulated conditions over time. Effects include:
Latent effects: Early exposures leave lasting biological imprints.
Pathway effects: Early conditions set trajectories for education, work, and health.
Cumulative effects: Disadvantages compound over time, even if circumstances improve later.
Social Comparison Perspective
Health inequalities arise not only from material deprivation but also from perceived social position. Feelings of shame, worthlessness, and envy can activate stress pathways, leading to poorer health even when basic needs are met.
Structural Inequities and Health
Gender, Race, and Disability
Structural inequities in gender, race, and disability status shape access to resources, employment, and health care. These inequities result in higher stress, reduced independence, and poorer health outcomes for marginalized groups.
Political Economy and Neoliberalism
Market-driven policies and globalization have led to reduced public resources, increased precarious work, and weakened social supports. These changes disproportionately harm disadvantaged groups and increase health inequalities.
Summary Table: Key International Indicators
Measure | Finland | Canada | US |
|---|---|---|---|
% Living in poverty (2022) | 3 | 18 | 34 |
Food security environment (2022) | 1 | 7 | 34 |
Income inequality (2022) | 7 | 14 | 36 |
Public social expenditure (2022) | 8 | 30 | 34 |
Life expectancy (2022) | 15 | 18 | 31 |
Child environmental well-being (2022) | 5 | 28 | 37 |
Conclusion
Understanding and addressing the social determinants of health is essential for reducing health inequalities and improving population health. Effective interventions require upstream, equity-focused policies that address the root causes of disadvantage and invest in social supports for all.
